Scope & Definitions
The NICE guideline NG126 covers diagnosis and initial management in women ≤ 13 completed weeks with pain or bleeding in early pregnancy. NICE
It replaces CG154 (2012). NICE
RCOG Green-top Guideline No. 21 addresses ectopic pregnancy diagnosis & management in detail. Royal College of Obstetricians+1
Also relevant: NICE / ACOG on early pregnancy loss (miscarriage) management. ACOG+1
Clinical presentation & initial assessment
History & risk factors
Common symptoms: vaginal bleeding, abdominal / pelvic pain (often between 6–10 weeks) PMC+1
Atypical presentations are possible (e.g. gastrointestinal symptoms, syncope). Clinicians must maintain suspicion in women of reproductive age with pain or bleeding. PMC+2NICE+2
Risk factors for ectopic pregnancy: prior tubal surgery, pelvic inflammatory disease, tubal damage, previous ectopic, ART/IVF, smoking, age > 35, prior pelvic/abdominal surgery.
Physical examination & vital signs
Assess hemodynamic stability: pulse, blood pressure, signs of shock/haemorrhage.
Abdominal tenderness, peritoneal signs.
Speculum/vaginal exam: bleeding source, cervical motion tenderness, adnexal tenderness or mass (but gentle – avoid provoking bleed).
Beware that some ectopics present with minimal signs; absence of classic signs does not exclude ectopic.
Diagnostic investigations
Serum ß-hCG & other biomarkers
A single ß-hCG at presentation is essential. Serial ß-hCG (e.g. 48-hour repeat) helps in distinguishing viability / rise patterns, especially in pregnancies of unknown location (PUL).
Serum progesterone is not recommended for diagnosing ectopic (poor discriminatory power) in routine practice.
 Ultrasound
Ultrasound
Transvaginal ultrasound (TVS) is the imaging modality of choice.
If TVS is inconclusive, can supplement with transabdominal.
Key sonographic findings favoring ectopic:
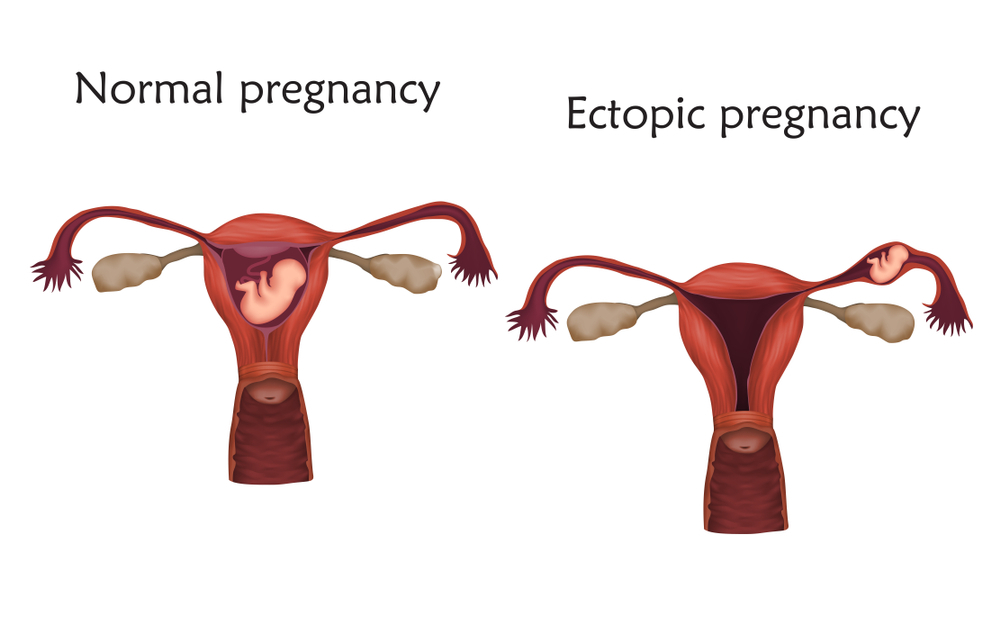
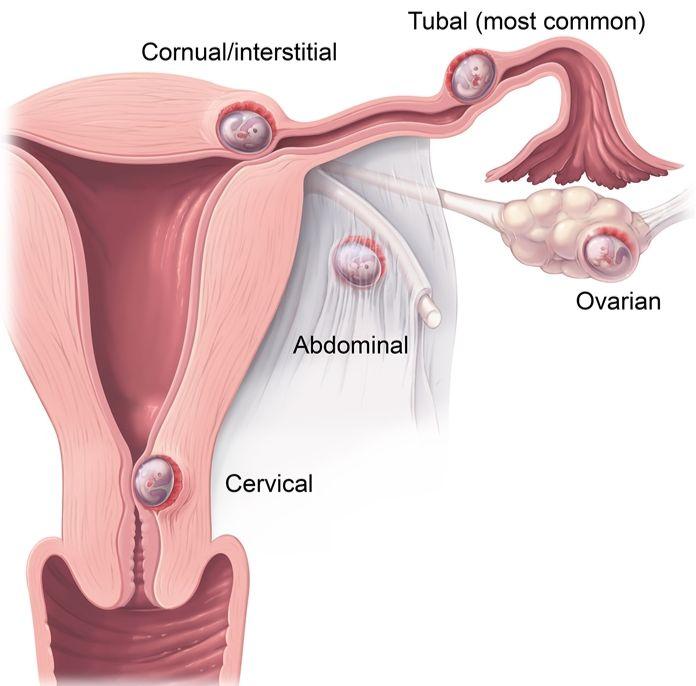
• Empty uterine cavity (no gestational sac)
• Adnexal mass / sac (separate from ovary) / “ring sign” / gestational sac with yolk sac / fetal pole outside uterus
• Free fluid in the pouch of Douglas (suggestive of bleeding)Other rarer ectopic types (cervical, caesarean scar, interstitial) have specific ultrasound criteria (e.g. interstitial line sign, myometrial thickness < 5 mm) TJO Istanbul+1
MRI may be adjunct if ultrasound equivocal and local expertise available. TJO Istanbul+1
Pregnancy of unknown location (PUL) algorithm
If neither IUP nor ectopic is visualized → label as PUL → follow with serial ß-hCG + repeat ultrasound until final diagnosis (viable IUP, failed PUL, or ectopic). TJO Istanbul+3PMC+3NICE+3
A PUL must be managed until definitive outcome – cannot prematurely treat as miscarriage without excluding ectopic. NICE+2ACOG+2
Distinguishing miscarriage (early pregnancy loss)
In confirmed intrauterine pregnancy, absence of fetal heartbeat or no growth on repeat scan suggests early pregnancy loss. ACOG+1
Only when confidently excluded ectopic, can management of miscarriage proceed (expectant, medical, surgical) NICE+1
Rh D prophylaxis: consider in miscarriage / early pregnancy loss (especially surgical) for Rh-negative women. ACOG+1
Initial management principles & decision-making
The goal is to choose the safest, least invasive option while preserving fertility, tailored to patient stability, size/viability of ectopic, and patient preferences.
When urgent surgical intervention is required
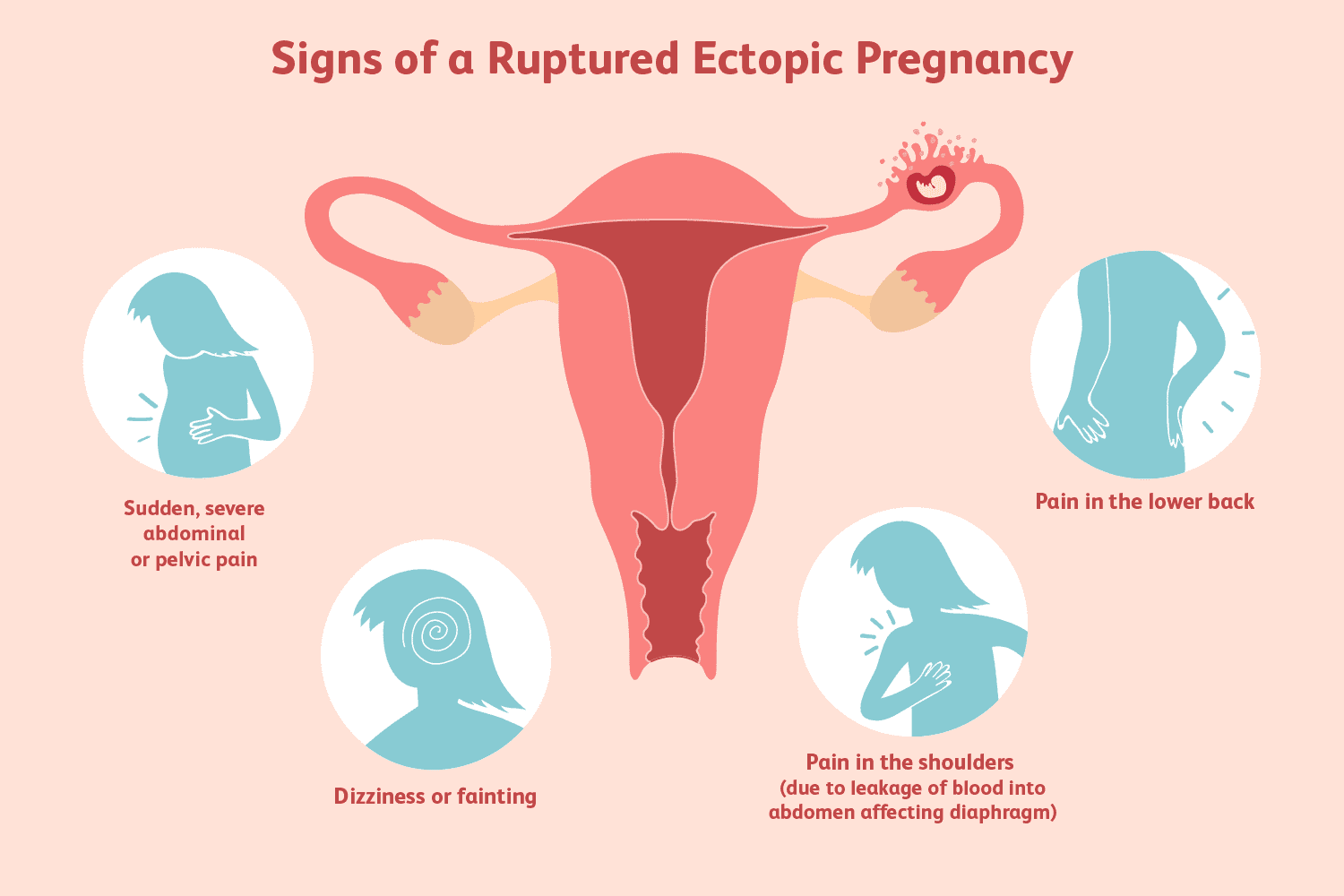
Hemodynamic instability, signs of rupture or acute abdomen → immediate surgical management.
If massive intraperitoneal bleeding suspected or peritoneal signs → laparotomy if unstable, or laparoscopy if stable enough.
In surgery, options include salpingectomy or salpingostomy (conservative) depending on condition, contralateral tube, and surgeon expertise.
Medical management (methotrexate)
Indications: stable patient, no signs of rupture, small ectopic mass (often < 3 – 4 cm, no significant free fluid), low and declining or modestly rising ß-hCG (often < 5000 IU/L, though thresholds vary)
Contraindications include: hemodynamic instability, coexisting viable IUP (heterotopic), high ß-hCG beyond safe limit, significant pain, large mass, contraindications to MTX (renal, hepatic disease, immunodeficiency)
Regimens: single-dose methotrexate (with folinic acid rescue) is commonly used; some centers use multi-dose regimens.Monitor ß-hCG after treatment (e.g. day 4, day 7). A fall ≥ 15% between days 4 & 7 suggests treatment success; if not, may need additional dose or surgery.
Close follow-up with serial ß-hCG until undetectable.
Expectant (conservative) management
Consider in selected patients with low, falling ß-hCG levels and minimal symptoms, and in whom spontaneous resolution is likely.
Requires rigorous follow-up (ß-hCG, repeat ultrasound).
Not appropriate if rising ß-hCG or risk of rupture.
Miscarriage (early pregnancy loss) management
Once ectopic is excluded:
Options: expectant, medical, or surgical evacuation. ACOG+1
Medical: Misoprostol (800 µg vaginal) is standard; adding mifepristone (200 mg) 24h before misoprostol improves efficacy. ACOG
Surgical: Vacuum aspiration / suction curettage as needed (e.g. heavy bleeding, incomplete loss). Use prophylactic antibiotics (doxycycline) and Rh immunoglobulin in Rh-negative women if surgical. ACOG+1
Expectant: In asymptomatic women with low risk of complications; monitor until complete expulsion.
Rh D prophylaxis: in miscarriage / surgical management in Rh-negative women (especially >6–12 weeks). ACOG+1
Follow-up, counseling & future pregnancies
Counsel patient regarding future fertility, risk of recurrence, timing of next pregnancy.
In next pregnancy, early ultrasound (first trimester) to confirm intrauterine location.
Psychological support, grief counseling as early pregnancy loss / ectopic has emotional impact.
Ensure adequate follow-up for ß-hCG to zero in ectopic cases.
Document and review risk factors to counsel and possibly modify (e.g. smoking cessation).
 Recommended management (per RCOG / NICE):
Recommended management (per RCOG / NICE):
If the patient is clinically stable, and the scan shows no intrauterine or ectopic mass,
→ Repeat serum hCG in 48 hours and reassess.Expected pattern:
Normal intrauterine pregnancy: hCG rises by ≥63% in 48 hours.
Failing pregnancy: hCG falls by ≥50%.
Ectopic pregnancy: hCG rise is suboptimal or plateauing.
Summary algorithm (simplified)
Woman presents with bleeding ± pain in early pregnancy ➝
Check vital signs → If unstable, manage as surgical emergency.
Draw ß-hCG, do transvaginal ultrasound.
If IUP confirmed → proceed to evaluate for viability / miscarriage.
If ectopic visualized → decide between surgery / methotrexate / expectant.
If PUL → serial ß-hCG + repeat ultrasound until final status determined.
Once ectopic excluded and intrauterine nonviable pregnancy, manage miscarriage (expectant / medical / surgical) with Rh prophylaxis as needed.
Miscarriage – Key Points
🔹 Definitions
Miscarriage: Pregnancy loss before 24 weeks (usually <20 weeks for RCOG context).
Threatened: Bleeding, closed os, live fetus.
Inevitable: Open os, ongoing bleeding.
Incomplete: Some products passed.
Complete: All products expelled, empty uterus.
Missed: Retained non-viable pregnancy, no bleeding.
🔹 Diagnosis
Transvaginal ultrasound is gold standard.
Crown–rump length (CRL) ≥7 mm with no heartbeat = miscarriage.
Mean gestational sac ≥25 mm with no embryo = miscarriage.
If uncertain, repeat scan after 7–10 days.
🔹 Management Options
1. Expectant management
Suitable if <13 weeks and clinically stable.
70–80% success within 2 weeks.
2. Medical management
Mifepristone 200 mg orally, then Misoprostol 800 µg vaginally after 24 hours.
Effective in 80–90%.
Can repeat misoprostol if incomplete.
3. Surgical management
Manual vacuum aspiration (MVA) or suction curettage.
Indications:
Heavy bleeding, infection, or patient preference.
Failed expectant/medical management.
🔹 Rh prophylaxis
Rh-negative women: give Anti-D 250 IU if
Surgical or medical evacuation
Ectopic pregnancy
≥12 weeks bleeding
Threatened miscarriage after 12 weeks
🔹 Post-miscarriage care
Provide written information and emotional support.
Offer follow-up ultrasound if symptoms persist.
Refer for recurrent miscarriage if ≥3 consecutive losses.
🧠 MRCOG Exam Tips
Know criteria for expectant vs methotrexate vs surgery in ectopic.
hCG thresholds and trends are frequent SBA themes.
For miscarriage: recall ultrasound criteria and Anti-D indications.
In TOACS: focus on counselling, safety-netting, and emotional support.
Always mention early scan in next pregnancy.