Definition
Hb < 11 g/dL (WHO definition)
Trimester-specific thresholds (RCOG / WHO):
1st trimester: Hb < 11 g/dL
2nd trimester: Hb < 10.5 g/dL
3rd trimester: Hb < 11 g/dL
Postpartum: Hb < 10 g/dL
🔹 Physiological (Dilutional) Anemia
Plasma volume ↑ by 40–50%
RBC mass ↑ by 20–30%
Result: hemodilution → mild anemia (Hb ~10–11 g/dL)
Normal iron stores = 500–1000 mg → pregnancy needs ~1000 mg iron total.
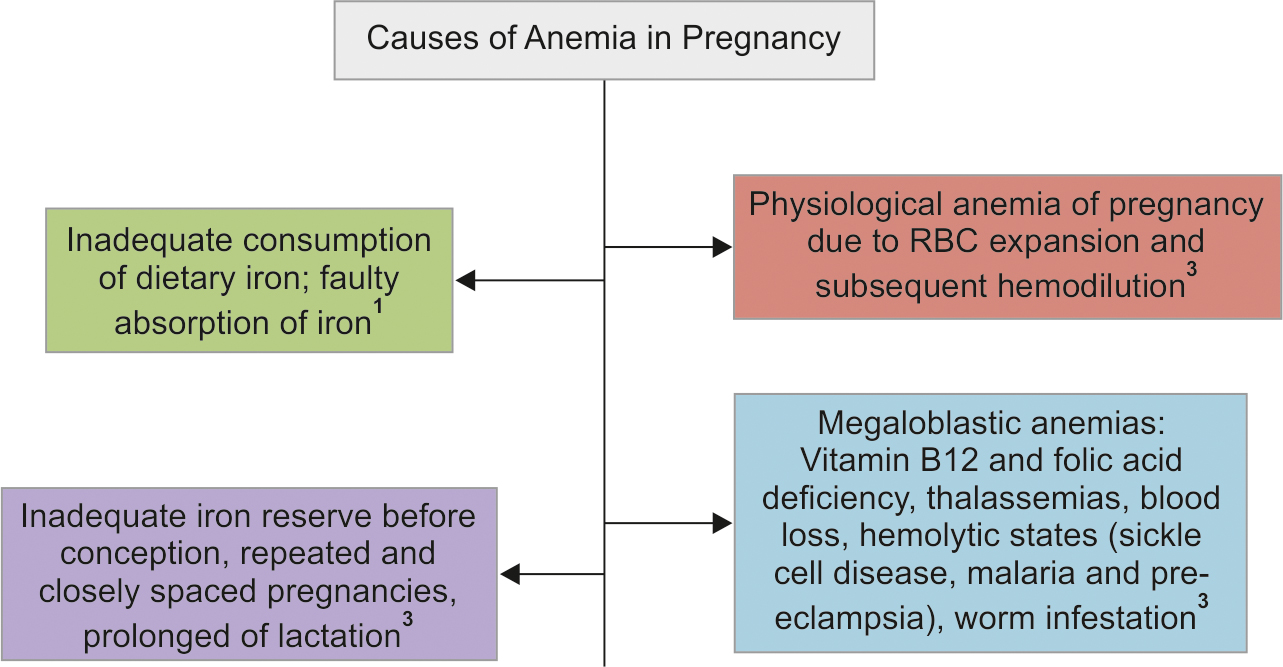
 🔹 Causes
🔹 Causes
Iron deficiency anemia (most common worldwide)
Folate deficiency
Vitamin B12 deficiency
Hemoglobinopathies (thalassemia, sickle cell disease)
Anemia of chronic disease, infection, or bone marrow suppression
🔹 Screening & Diagnosis
Routine antenatal screening:
Hb at booking and at 28 weeks
If Hb low → check:
MCV, MCH
Serum ferritin (best indicator of iron stores)
< 30 µg/L → iron deficiency
Peripheral smear for morphology
Hb electrophoresis if MCV low and not iron deficient (to rule out thalassemia)
 🔹 Classification (by Hb level)
🔹 Classification (by Hb level)
| Severity | Hb (g/dL) |
|---|---|
| Mild | 10–10.9 |
| Moderate | 7–9.9 |
| Severe | < 7 |
| Very severe | < 4 |
🔹 Maternal Complications
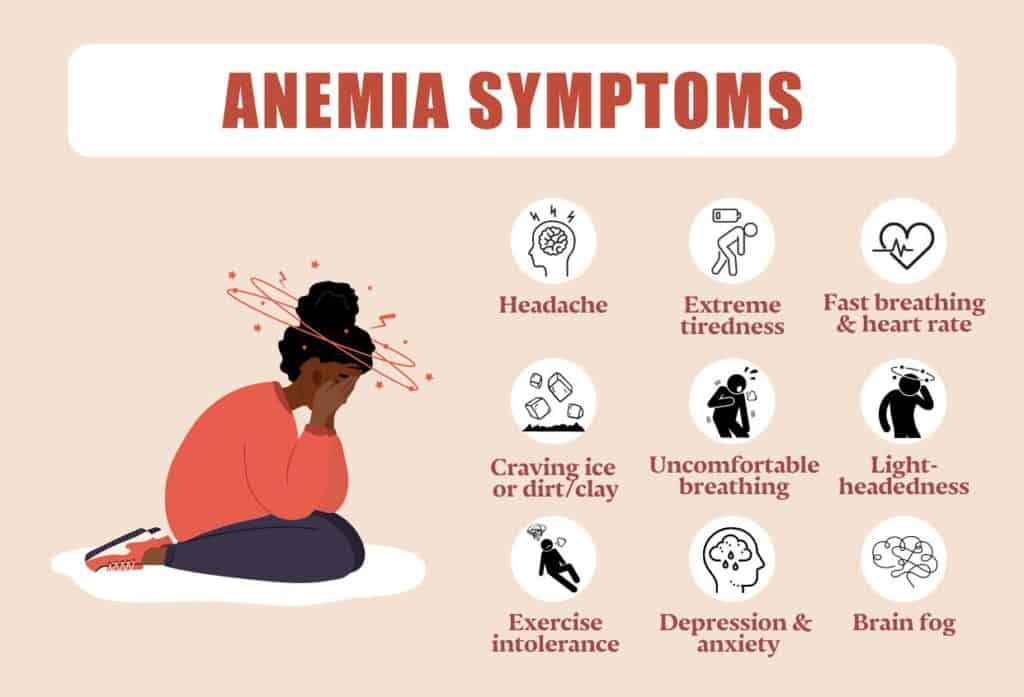
Fatigue, infections, pre-eclampsia
Heart failure, shock during labour
Poor wound healing
Postpartum hemorrhage
🔹 Fetal Complications
IUGR, preterm birth, low birth weight
Perinatal mortality
Fetal hypoxia and poor iron stores
 🔹 Management
🔹 Management
🩺 General Principles
Identify cause (iron, folate, B12, etc.)
Treat underlying cause
Monitor response (Hb rise ≥1 g/dL in 2–3 weeks)
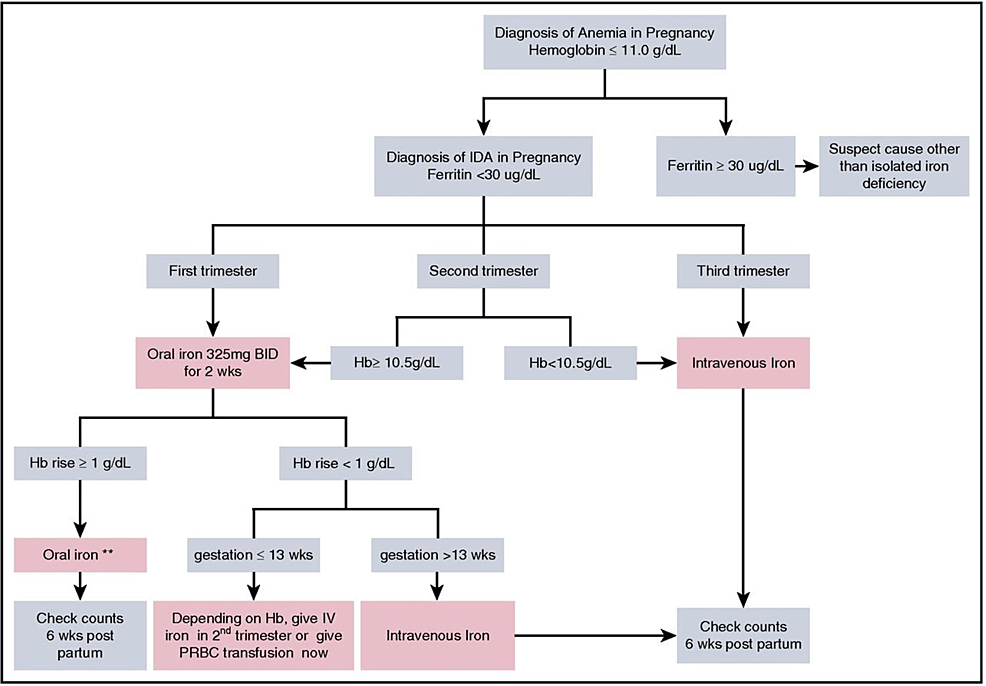
1. Iron Deficiency Anemia
Oral Iron:
Ferrous sulfate 200 mg TDS (provides ~60 mg elemental iron/tablet)
Continue for 3 months after Hb normalization
Add folic acid 400 µg daily
Side effects: GI upset, constipation → switch to ferrous fumarate/gluconate or alternate days.
Parenteral Iron Indications:
Intolerance to oral iron
Poor compliance or absorption
Late pregnancy with moderate–severe anemia
Hb < 8 g/dL after 30 weeks
Preparations: Iron sucrose, ferric carboxymaltose, iron dextran (less used)
2. Folate Deficiency
Folic acid 5 mg/day during pregnancy
Preventive dose: 400 µg/day preconception–12 weeks
3. Vitamin B12 Deficiency
Hydroxocobalamin 1 mg IM 3×/week for 2 weeks, then every 3 months
4. Severe Anemia (Hb < 7 g/dL)
Hospital admission
Investigate cause
Consider blood transfusion if:
Hb < 7 g/dL (symptomatic or near term)
Hb < 8 g/dL with cardiac failure or delivery imminent
Preoperative for C-section or PPH risk
🔹 Prevention
Routine iron + folate supplementation to all pregnant women
Iron 60 mg + folic acid 400 µg daily
Deworming in endemic areas
Treat malaria, hookworm
Adequate nutrition and spacing of pregnancies
🔹 Postpartum Care
Continue oral iron for 3 months postnatally
Treat cause if persists
If severe → transfusion or parenteral iron
Definition (WHO)
Hb < 11 g/dL in pregnancy
Mild: 10–10.9 g/dL
Moderate: 7–9.9 g/dL
Severe: <7 g/dL
 Causes
Causes
Nutritional deficiency
Iron deficiency (most common)
Folate or Vitamin B12 deficiency
Blood loss
Antepartum or postpartum hemorrhage
Hemoglobinopathies
Thalassemia, sickle cell disease
Chronic disease
Renal, infections (malaria, hookworm, etc.)
Physiological Changes
Plasma volume ↑ 50%
RBC mass ↑ 20–30%
→ Physiological hemodilution → mild anemia (~10–10.5 g/dL normal)
Diagnosis
Initial screening: Hb at booking & at 28 weeks.
Investigations:
CBC, MCV, MCH
Peripheral smear
Ferritin, serum iron, TIBC
Folate, B12 if indicated
Hb electrophoresis if microcytic not due to iron deficiency
Iron Deficiency Anemia
Most common cause
Ferritin < 30 µg/L diagnostic
Microcytic, hypochromic picture
Treatment:
Oral iron: Ferrous sulfate 200 mg TDS (contains ~60 mg elemental iron)
Add folic acid: 5 mg daily
Duration: Continue for 3 months after Hb normalization
If oral not tolerated or ineffective: IV iron (e.g., ferric carboxymaltose)
Folate Deficiency
Megaloblastic anemia, MCV ↑
Folic acid 5 mg/day throughout pregnancy for prevention/treatment
Severe Anemia (Hb <7 g/dL)
Assess cause + stability
Management:
Admit, monitor vitals
Transfuse packed RBCs if symptomatic or near term
Correct cause with iron/folate
Intrapartum:
Crossmatch blood
Minimize blood loss (active management of 3rd stage)
Oxygen, avoid supine hypotension
Postpartum:
Continue supplementation
Evaluate for chronic cause
Complications
Maternal:
Preterm labor, PPH, infection, cardiac failure, poor lactation
Fetal:
IUGR, preterm, low birth weight, perinatal death, poor oxygenation
Prevention
Routine iron + folate supplementation from booking
Deworming (where endemic)
Nutrition counseling
Birth spacing
Key TOACS Tips
🔹 Common station types:
Counseling station: counsel a pregnant woman with moderate anemia at 32 weeks
Data interpretation: CBC with low Hb & MCV
Management plan: pre-labor severe anemia
Communication: explaining iron therapy, side effects, diet advice
Sample Counseling Points
“Your blood level is low because of iron deficiency, which is common in pregnancy.
We’ll start you on iron tablets and folic acid. Take them with orange juice, avoid tea or coffee near the time you take your tablets.
This will help improve your blood level and reduce risks to you and your baby.”
References
WHO: Guideline on Iron Supplementation in Pregnancy (2023)
NICE NG201: Antenatal Care (2021)
RCOG GTG No. 47: Blood Transfusions in Obstetrics
Parkland & DC Dutta’s Textbook of OBGYN (for FCPS prep)
For Ready-to-practice FCPS TOACS role-play dialogue on Anemia in Pregnancy click below