Endometriosis is a clinical diagnosis based on history and exam; imaging (TVS/MRI) is used to identify endometriomas or deep disease, and diagnostic laparoscopy is no longer required purely to make the diagnosis in uncomplicated cases. NICE+1
First-line care = analgesia + empirical hormonal therapy (combined oral contraceptive pill, progestogens including LNG-IUS, or norethisterone) for pain control in those not seeking immediate pregnancy. Consider trial of medical therapy for 3 months. NICE+1
Use pelvic transvaginal ultrasound (TVS) as first-line imaging to detect ovarian endometrioma; MRI is helpful when deep (rectovaginal/parametrial) disease or complex anatomy is suspected. Do not rely on ultrasound to rule out all disease. NICE+1
Surgery (laparoscopic excision/ablation) is indicated when pain is refractory to medical therapy, when anatomical distortion or endometrioma compromises fertility, or where deep disease causes organ symptoms — but surgery must balance symptom benefit vs. risk to ovarian reserve (especially for endometriomas). Conservative fertility-preserving techniques are preferred. RCOG+1
Fertility approach: if trying to conceive, manage jointly with fertility services. For many women with minimal/mild disease, expectant management or assisted conception (IUI/IVF) may be preferred to repeated surgery; removal of asymptomatic endometriomas before IVF is generally avoided because surgery can reduce ovarian reserve. Refer early if conception not achieved within 6–12 months (age-dependent). NICE+1
Detailed exam-style summary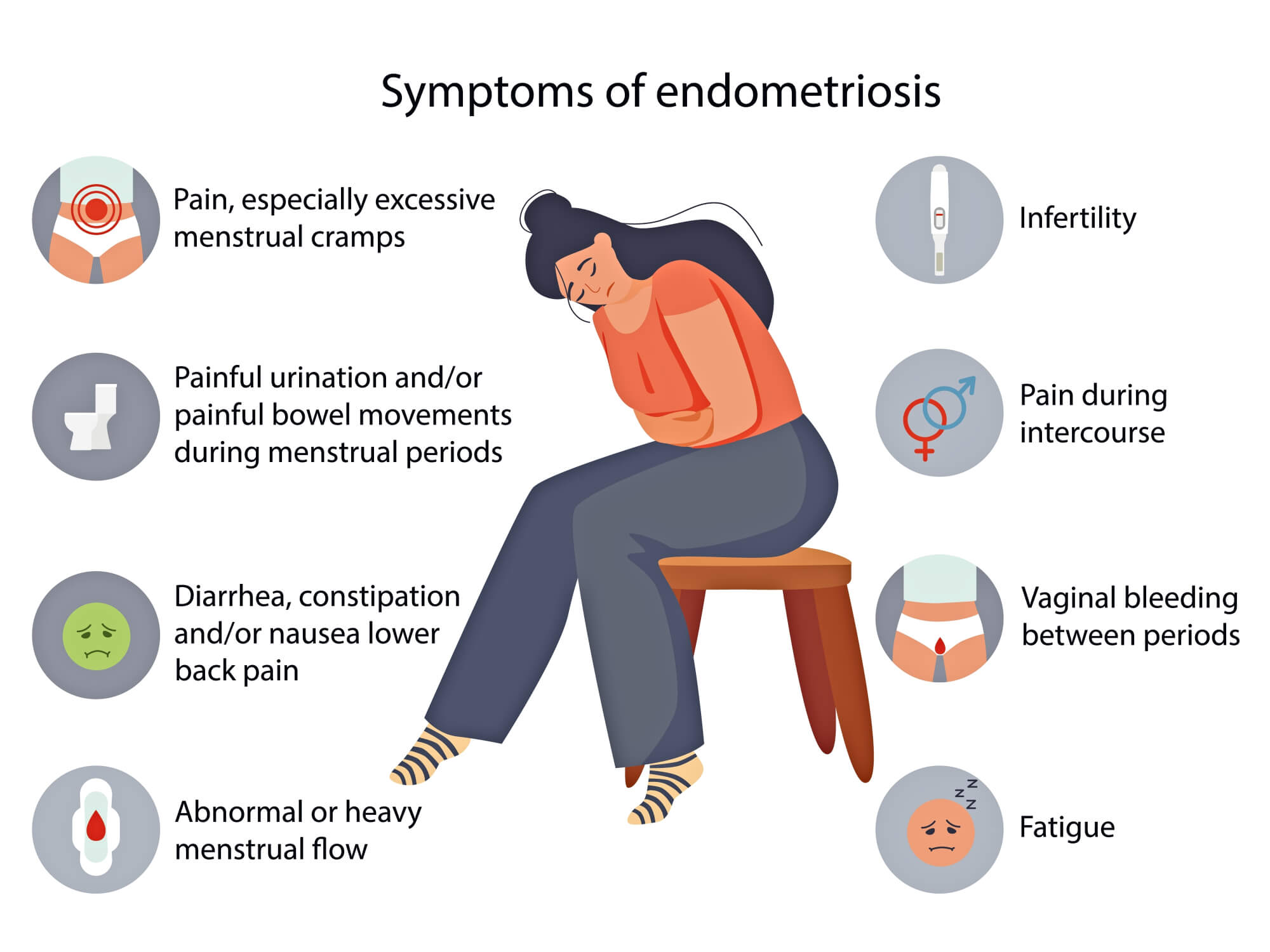
1) Epidemiology & presentation — quick facts
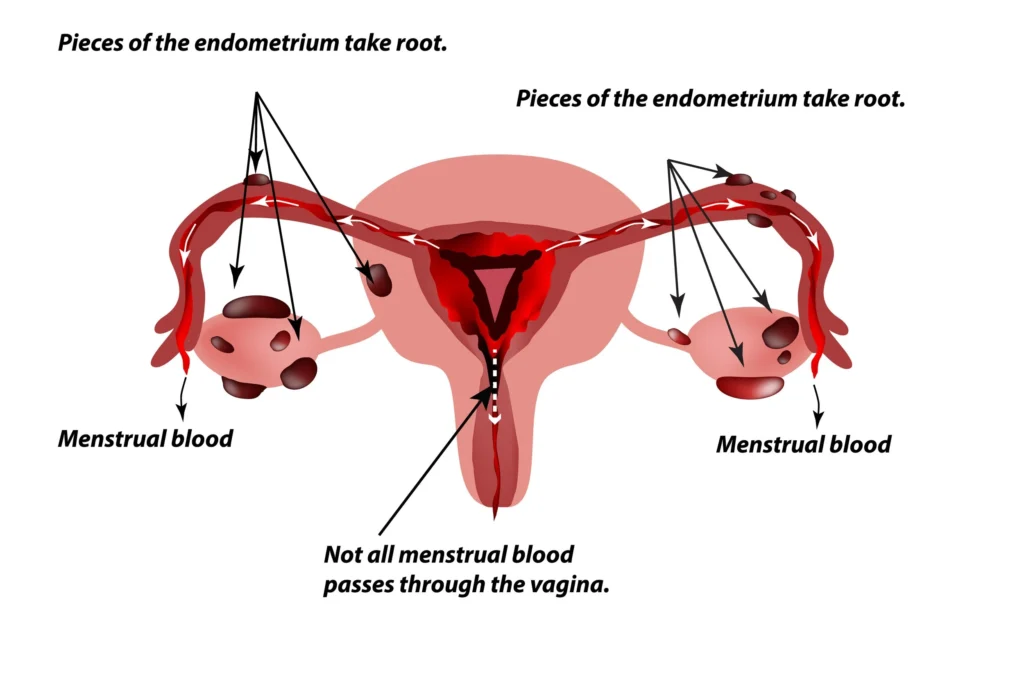
Typical age: reproductive years (often 25–45). Classic triad: dysmenorrhoea, deep dyspareunia, chronic pelvic pain; also subfertility, cyclical bowel/urinary symptoms. PMC
Delay to diagnosis in real world is long (many years) — be alert to severity and impact on quality of life. endometriosis-uk.org
2) Initial assessment (history & exam) — what exams test
Focused history: cyclical pattern, bowel/urinary symptoms, infertility history, prior surgery, contraceptive use, analgesic response.
Exam: abdominal, speculum, bimanual — look for fixed retroverted uterus, adnexal masses (endometrioma), tenderness. Rectovaginal exam if deep dyspareunia or suspected deep disease. NICE
3) Essential investigations
Pregnancy test (exclude).
Transvaginal pelvic ultrasound (TVS): first-line for adnexal masses/endometrioma; targeted scan for DIE (deep infiltrating endometriosis) if operator experienced. NICE
MRI pelvis: use when TVS is inconclusive or to map deep/rectovaginal disease, plan complex surgery. ESHRE
Bloods: FBC if heavy bleeding/anaemia; CA-125 is not diagnostic and should not be used as a screening test but may be elevated and occasionally used in monitoring in specific contexts (not routine). NICE
Laparoscopy: reserved for when surgery is planned or diagnosis is unclear after non-invasive methods; diagnostic laparoscopy purely to confirm disease is not required in many cases. NICE+1
4) Medical management — exam high yield
Analgesia: NSAIDs ± paracetamol; consider neuropathic agents for chronic pelvic pain.
Hormonal options (choose based on fertility desire & comorbidities):
Combined oral contraceptive pill (COCP) — continuous use can reduce dysmenorrhoea.
Progestogens (oral norethisterone, dienogest): effective for pain.
Levonorgestrel-IUS (LNG-IUS): very useful for heavy bleeding and pelvic pain.
GnRH agonists (with add-back HRT): effective short-term (e.g., for 3–6 months) but consider bone/menopausal effects and cost.
Trial length: usually 3 months to assess effectiveness; switch if inadequate. Stop if wanting pregnancy. NICE+1
5) Surgical management — what to know for exams
Indications: refractory pain despite optimal medical therapy, endometrioma causing pain or interfering with fertility, hydronephrosis/ureteric involvement, severe rectal/urinary symptoms from DIE, diagnostic uncertainty or mass suspicion of other pathology. ESHRE
Approach: laparoscopic excision (removal of lesions & adhesiolysis) is preferred for pain relief and fertility benefit in many cases; segmental bowel/ureteric surgery for deep disease should be multidisciplinary.
Endometrioma management: cystectomy (stripping) reduces recurrence and pain but may lower ovarian reserve. Consider cyst fenestration/ablation or conservative surgery depending on size, symptoms, and fertility plans. Preoperative counselling on AMH/ovarian reserve is essential. RCOG
Postoperative hormonal therapy may reduce recurrence of pain but does not necessarily improve fertility outcomes — tailor to patient. NICE
6) Fertility & reproductive options
If trying to conceive: avoid empirical long courses of surgery that could reduce ovarian reserve unless pain/anatomical factors justify it. Consider assisted reproductive technologies (ART) earlier in older women or after 6–12 months of trying, depending on age and ovarian reserve. Multidisciplinary fertility referral recommended. NICE+1
7) Multidisciplinary care & long-term issues
Refer to pelvic pain services, specialist endometriosis centres for complex/deep disease. Psychological support and physiotherapy (pelvic floor) useful adjuncts. Screen and optimise bone health if using prolonged GnRH therapy. NICE
8) Special situations — quick points
Adolescents: avoid diagnostic laparoscopy solely for diagnosis; consider hormonal suppression early for pain control.
Pregnancy & endometriosis: pregnancy does not reliably cure endometriosis; manage symptoms appropriately.
Malignancy risk: small but present — suspicious masses require imaging and surgical evaluation. PMC
One-page Quick-Sheet for Exams (memorise these lines)
Dx = clinical + TVS/MRI for mapping; laparoscopy only if planning surgery or unclear. NICE
First line: NSAIDs + hormonal therapy (COCP/progestogens/LNG-IUS/dienogest). Trial 3 months. NICE
Indications for surgery: refractory pain, endometrioma with symptoms, fertility problems, organ compromise. ESHRE
Endometrioma surgery reduces recurrence but may reduce ovarian reserve — counsel and consider fertility preservation. RCOG
Refer to specialist centre for DIE, multidisciplinary management (urology/colorectal/reproductive surgery). ESHRE
10 Rapid exam-flashcards (Q → A, memorise)
Q: First-line imaging for suspected endometrioma?
A: Transvaginal ultrasound (TVS). NICEQ: Is CA-125 diagnostic for endometriosis?
A: No — not used as a screening/diagnostic test. NICEQ: Next step for a woman with pelvic pain who wants fertility and has a 4 cm endometrioma?
A: Discuss risks/benefits — consider conservative surgery if symptomatic or interfering with ART, otherwise consider fertility treatment and counsel re ovarian reserve. RCOGQ: Medical options to suppress endometriosis pain if pregnancy not desired?
A: COCP (continuous), oral progestogens, LNG-IUS, dienogest, or GnRH agonist (short term). NICEQ: Role of laparoscopy for diagnosis?
A: Not required solely for diagnosis if clinical + imaging suffice; laparoscopy used when surgery is considered. NICEQ: Best management for deep infiltrating endometriosis involving rectum?
A: Multidisciplinary surgical planning (colorectal/urology + gynaecology) at specialist centre. ESHREQ: Should all endometriomas be removed before IVF?
A: No — asymptomatic endometriomas are often left alone because surgery may reduce ovarian reserve; individualise decision. RCOGQ: Post-op medical therapy prevents recurrence?
A: Post-op suppression can reduce recurrence of pain but does not guarantee improved fertility; individualise. NICEQ: When to refer to specialist endometriosis service?
A: Complex/deep disease, recurrent severe symptoms, organ involvement, or fertility issues needing multidisciplinary care. ESHREQ: Young patient with severe dysmenorrhoea — next step?
A: Start trial of hormonal suppression + analgesia; avoid early diagnostic laparoscopy unless red flags or failure of therapy. NICE
Useful reference links (guideline sources I used)
RCOG: Endometriosis — Investigation & Management (Green-top page & patient info). RCOG+1
NICE NG73: Endometriosis: Diagnosis and Management (national guidance). NICE
ESHRE Guideline: Management of women with endometriosis (2022). ESHRE
RCOG Scientific impact paper on endometrioma surgery & fertility. RCOG
Click below for ESHRE and Nice Guidelin pdf