Nausea and vomiting are extremely common in early pregnancy, but when the symptoms become severe, persistent, and debilitating, the condition is known as Hyperemesis Gravidarum (HG). The Royal College of Obstetricians and Gynaecologists (RCOG) recently updated its Green-top Guideline No. 69 (2024), offering clearer, evidence-based recommendations on diagnosis and management.
This blog breaks down the guideline into simple, practical points for healthcare providers, students, and mothers alike.
Hyperemesis Gravidarum: More Than Just Morning Sickness
Many people think nausea and vomiting in pregnancy are simply “morning sickness,” a common and expected part of early pregnancy. However, Hyperemesis Gravidarum (HG) is very different. According to the Royal College of Obstetricians and Gynaecologists (RCOG), HG affects up to 3% of pregnancies and is considered a serious medical condition, not a normal variation of pregnancy symptoms.
 How HG Differs From Morning Sickness
How HG Differs From Morning Sickness
Morning sickness:
Common, mild to moderate nausea
Usually improves by 12–14 weeks
Women can generally eat, drink, and function normally
Hyperemesis Gravidarum:
Persistent and severe nausea and vomiting
Inability to keep down food or fluids
>5% weight loss from pre-pregnancy weight
Dehydration and electrolyte imbalance
Can continue well into the second or even third trimester
Often requires medical treatment, IV fluids, and antiemetics
Why HG is a Serious Condition
HG can lead to significant complications for the mother if not managed properly:
Severe dehydration
Nutritional deficiencies
Wernicke’s encephalopathy (due to thiamine deficiency)
Hospitalisation
Blood clots (due to immobility and dehydration)
Psychological impact — anxiety, depression, and social isolation
It also affects daily life — women may be unable to work, care for themselves, or manage household responsibilities.
Impact on Baby
While most babies are born healthy when HG is treated early and effectively, uncontrolled or prolonged HG may contribute to:
Low birth weight
Preterm birth (rare but possible)
Reduced maternal weight gain affecting fetal growth
Why Awareness Matters
Many women with HG feel dismissed or misunderstood because symptoms resemble morning sickness. RCOG emphasises the importance of:
Recognising HG early
Taking symptoms seriously
Providing timely treatment
Offering emotional support
 This improves outcomes and reduces the emotional and physical burden on women.
This improves outcomes and reduces the emotional and physical burden on women.
⭐Understanding the Spectrum: NVP vs. HG
NVP – Nausea and Vomiting of Pregnancy
NVP includes mild to moderate nausea and vomiting that usually starts in the first trimester. It is common and typically manageable.
HG – Hyperemesis Gravidarum
HG is a severe form of pregnancy sickness, characterised by:
Persistent/prolonged nausea and vomiting
>5% pre-pregnancy weight loss
Dehydration
Electrolyte imbalance
Inability to tolerate oral intake
Importantly, RCOG now clarifies that ketonuria (ketones in urine) is NOT a reliable marker of severity and should not be used alone for diagnosis.
⭐ Tools to Assess Severity
The updated guideline encourages using validated scoring tools:
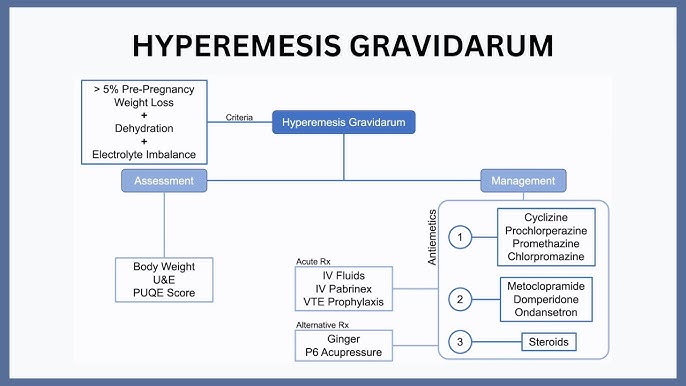
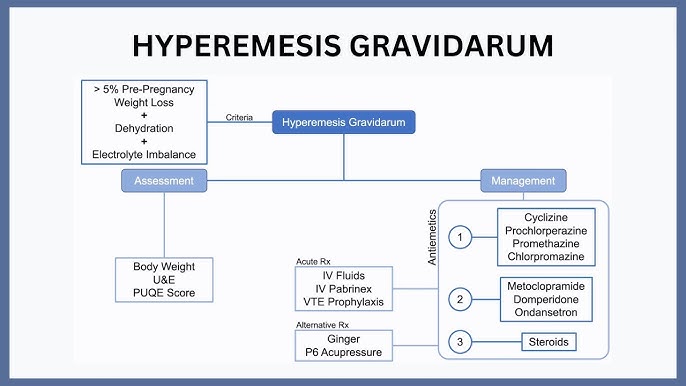
1. PUQE Score (Pregnancy-Unique Quantification of Emesis)
Assesses vomiting, retching, and nausea over the previous 24 hours.
2. HELP Score (HyperEmesis Level Prediction)
More comprehensive; helps monitor treatment response and predict need for hospitalisation.
These tools improve standardisation and prevent missing severe cases.
⭐ First-Line Management (Community Care)
For women with mild symptoms:
✔ Lifestyle/dietary modification (small meals, ginger products)
✔ Oral antiemetics considered SAFE in pregnancy:
Antihistamines: cyclizine, promethazine, dimenhydrinate
Doxylamine + Pyridoxine combination (first-line in many countries)
Phenothiazines: prochlorperazine, chlorpromazine
The guideline emphasises early initiation of antiemetics to prevent deterioration.
⭐ When to Step Up Care
Patients should be escalated from community to day-care/hospital care when they have:
Weight loss >5% of pre-pregnancy weight
Inability to tolerate oral food/fluids
Recurrent vomiting despite oral medications
Signs of dehydration
Electrolyte imbalance
Coexisting infection, thyroid disease, or other complicating factors
⭐ Ambulatory (Day-Care) Management
This is recommended for women with persistent symptoms but not needing admission.
Typical care includes:
✔ IV fluids (Normal Saline ± Potassium)
✔ IV antiemetics
✔ Thiamine administration
✔ Monitoring PUQE/HELP scores
It allows safe care while reducing inpatient burden.
 ⭐ Inpatient/Hospital Management
⭐ Inpatient/Hospital Management
Hospital admission is required when the woman is:
Clinically dehydrated
Unable to tolerate oral/ambulatory treatment
Severely malnourished
Showing electrolyte abnormalities
At risk of complications
Hospital Management Includes:
1. IV Fluid Therapy
Normal saline is preferred
Add potassium as needed
Give IV Thiamine before any dextrose to prevent Wernicke’s encephalopathy
2. Combination Antiemetic Therapy
If single agents fail, combine different classes:
Antihistamines
Phenothiazines
Ondansetron (second-line but accepted and supported by updated evidence)
3. Corticosteroids
Reserved for refractory cases after all other antiemetic regimens have failed.
4. Thromboprophylaxis
HG increases thrombosis risk – use LMWH if immobile/hospitalised.
5. Nutritional Support
Dietitian referral
Enteral feeding (NG/NJ tubes) if poor intake persists
TPN only when all other options fail
⭐ Impact on Mothers & Families
HG can severely affect:
Quality of life
Ability to work
Family responsibilities
Emotional well-being
Risk of anxiety/depression
The guideline encourages clinicians to take symptoms seriously and provide early, compassionate care.
⭐ Key Take-Home Messages
HG is not just “bad morning sickness”; it is a potentially serious condition.
Diagnosis should rely on clinical features and scoring tools, not ketones.
Early antiemetic treatment prevents complications.
Ambulatory care is effective for moderate cases.
Severe HG requires holistic hospital-based management including fluids, electrolytes, thiamine, and safe antiemetics.
Mental health support is essential.
⭐ Conclusion
The updated RCOG guideline offers clearer, stronger, and more patient-centred recommendations for managing hyperemesis gravidarum. The emphasis on early recognition, objective scoring, safe medications, and multidisciplinary care ensures women receive the support they need.
Raising awareness can help reduce stigma, prevent complications, and improve outcomes for pregnant women facing this challenging condition.
The Management of Nausea andVomiting of Pregnancy and Hyperemesis Gravidarum Green-top Guideline No. 69