4. Breech Delivery — (Exam-Focused Summary)
1) Epidemiology
Breech = longitudinal lie with buttocks or feet presenting.
~3–4% of term singleton pregnancies.
More common preterm (~25% at 28 weeks; many turn spontaneously).
Associated with prematurity, uterine/fetal anomalies, placenta praevia, poly/oligohydramnios.
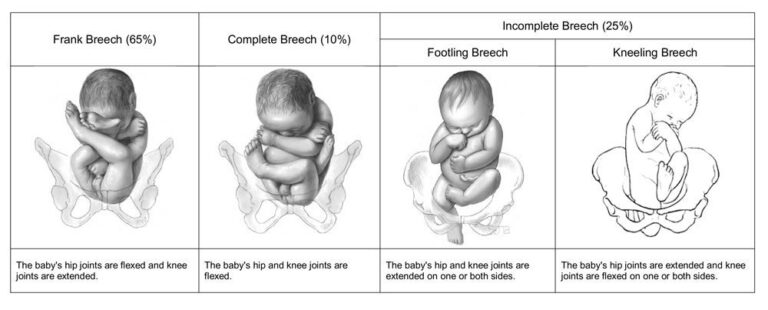
2) Types of breech
Frank (65%): hips flexed, knees extended (buttocks first).
Complete (25%): hips flexed, knees flexed (sitting).
Footling/incomplete (10%): one/both hips extended, foot presenting (↑ risk cord prolapse).
3) Antenatal Management
External Cephalic Version (ECV) – cornerstone
Timing: 36 weeks (nulliparas), 37 weeks (multiparas).
Success rate: ~40% nullips, ~60% multips.
Contraindications: placenta praevia, antepartum haemorrhage, abnormal CTG, multiple pregnancy (except 2nd twin), uterine scar is not absolute contraindication (counsel).
Adjuncts: tocolysis (terbutaline) improves success; anti-D if Rh–.
Complications: rare (<1%) – transient FHR abnormality, vaginal bleed, emergency CS.
Offer to all women with singleton breech at term unless contraindicated.
4) Mode of Delivery – key GTG recommendations
Planned CS reduces perinatal/neonatal morbidity & mortality compared to planned vaginal breech birth (Term Breech Trial, 2000).
But: absolute risk small; long-term neurodevelopment similar.
Planned vaginal breech delivery (VBD) remains an option in carefully selected women with appropriate expertise.
Selection criteria for VBD:
Term singleton, frank or complete breech.
No hyperextension of fetal head.
Estimated fetal weight 2.5–3.8 kg.
No antenatal evidence of fetopelvic disproportion.
Facility with skilled operator, continuous fetal monitoring, immediate CS capability.
5) Intrapartum Management of Vaginal Breech
Care principles:
Continuous CTG.
IV access, blood available.
Upright/lithotomy acceptable – many centres support upright (all-fours).
Avoid induction; cautious augmentation.
Second stage:
Passive descent → active pushing.
If breech not visible after 60 mins pushing → CS.
Key manoeuvres to know for MRCOG:
Pinard manoeuvre → flex & deliver extended legs.
Lovset manoeuvre → rotation & delivery of extended arms.
Mauriceau-Smellie-Veit (MSV) or forceps → control after-coming head.
Burns–Marshall method (less favoured today).
6) Special Situations
Preterm breech: ↑ risks; delivery mode individualized. Vaginal possible if spontaneous & imminent, but CS usually considered.
Second twin breech: often acceptable vaginally if first twin delivered cephalic, provided obstetrician skilled.
Footling breech: usually CS (risk cord prolapse).
Hyperextended head: contraindication to VBD.
7) Counselling Points (exam scenarios)
Discuss risks/benefits of planned CS vs VBD.
Document informed decision.
Re-offer ECV if not yet attempted.
Ensure intrapartum skilled support if VBD chosen.
8) Key Statements (memorise)
Offer ECV to all at term unless contraindicated.
Planned CS recommended, but VBD reasonable with strict criteria.
Vaginal breech should only be managed by trained/skilled clinicians.
Antenatal counselling must cover risks, benefits, recurrence (10%), and mode of delivery in future pregnancies.
9) Exam Tips
MRCOG SAQ: “Discuss management of term breech.” → structure: confirm, ECV, CS vs VBD counselling, intrapartum selection & monitoring, manoeuvres.
SBA/EMQ: likely to test ECV contraindications, manoeuvres, intrapartum complications (cord prolapse, head entrapment), counselling points.
📌 In summary (take-home for exam):
ECV = first-line at term.
Planned CS safer, but planned VBD is acceptable if strict criteria + skilled team.
Know manoeuvres (Pinard, Lovset, MSV).
Counselling & documentation are critical.
- Click below to attempt SBA/EMQs realted to this topic 👇