1. Gossypiboma and its Implications
Definition & Nomenclature
Gossypiboma (also called textiloma) refers to a retained surgical sponge, gauze, or cotton material inadvertently left inside the patient during surgery.
The term comes from gossypium (Latin for cotton) + boma (Swahili for place of concealment).
Epidemiology & Risk Factors
The true incidence is unknown (due to underreporting for medico-legal reasons) but estimated in abdominal surgeries as 1 per 1,000 to 15,000 operations.
It occurs more often after intra-abdominal and gynaecological/obstetric procedures.
Risk factors include:
Emergency or urgent operations
Hemorrhagic or difficult surgeries
Change of personnel during surgery
Large body habitus / obesity
Long surgical duration
Multiple surgical packs used
Inadequate sponge/instrument count procedures
Pathophysiology & Types of Reaction
When a sponge is retained, two broad types of corporeal reactions may happen:
Exudative / Inflammatory (Septic) Reaction
Leads to abscess formation, possibly with infection.
Presents earlier due to symptoms (fever, pain, discharge)
Aseptic / Fibrotic Reaction (Granulomatous Encapsulation)
The sponge becomes encapsulated by fibrous tissue and adhesions, forming a mass-like lesion (pseudo-tumor).
This may remain silent for years before detection.
The interval between the initial surgery and diagnosis may range from a few days up to 20 years (or more).
Clinical Presentation
Because of variable timing and reaction types, presentation is variable and non-specific:
Symptoms: Pain, fever, abdominal distension, mass, nausea, vomiting, bowel obstruction symptoms.
Signs: Palpable abdominal mass, signs of abscess, peritonitis, fistula formation. PMC+1
In pregnancy, a gossypiboma may mimic an adnexal mass or tumor on imaging.
Case example: One case report described gossypiboma in a patient at 38 weeks’ gestation, mimicking an ovarian neoplasm; the retained sponge was removed at cesarean section.
Diagnosis
Diagnosis is often delayed due to low suspicion, variable presentation, and medico-legal concerns. Key diagnostic approaches:
Imaging modalities:
X-ray (if sponge has radiopaque marker)
Ultrasound (may show an echogenic mass with shadows)
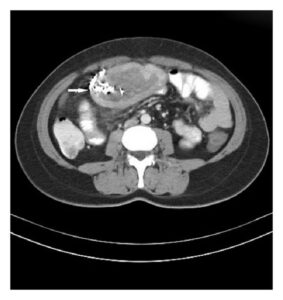
CT scan (often shows spongiform mass, internal gas bubbles, “whirl” or mottled pattern)
MRI / other advanced imaging in select cases.
Clinical suspicion: In any postoperative patient with unexplained pain, fever, mass or obstruction, retained surgical item should be in the differential.
Intraoperative exploration if imaging and suspicion strong.
Management
Surgical removal is the definitive treatment—usually via laparotomy, sometimes laparoscopically, depending on location and complexity.
Drainage of abscess (if present), debridement, and irrigation.
Postoperative care: antibiotics, monitoring for complications.
In pregnancy, removal is done at the time of cesarean or depending on stability and gestational age.
Complications & Implications
Morbidity: Adhesions, bowel obstruction, perforation, fistulae, abscess formation, sepsis, prolonged hospital stay, multiple reoperations.
Mortality: Rare but possible in severe cases with sepsis or multi-organ complications.
Legal / Medico-legal: High risk of litigation, reputational damage, medical negligence claims.
Emotional / Ethical: Loss of trust, ethical breach, psychological impact on patient and team.
Cost: Increased cost of care, re-operations, imaging, prolonged hospitalization.
Prevention (Key for MRCOG / Practical)
Since prevention is better than cure, these are high-yield:
Strict sponge/instrument counting protocols
Count at opening, before closure, and after wound closure.
Additional counts when personnel change or in emergencies.
Use of radiopaque markers on surgical sponges / packs so they show up on imaging if count discrepancy.
Minimize use of small sponges that can hide; use large, easily trackable packs.
Team communication & surgical safety checklists (such as WHO Surgical Safety Checklist) with “sponge count” as a mandatory element.
Surgeon’s manual exploration of cavity before final closure to ensure no retained items.
Bar-coding / RFID / technological adjuncts (in advanced settings) to track surgical sponges.
MRCOG-Relevant Points / Tips for Answering in Exams
In a scenario of postoperative fever, pain, or obstruction, always include retained surgical item (gossypiboma) in differential, especially after abdominal or obstetric surgery.
Know that diagnosis is often delayed, and imaging features (CT with spongiform pattern) are helpful.
Emphasize prevention, surgical safety protocols, counting, radiopaque markers, checklists.
If asked about legal / ethical implications, mention patient harm, litigation, loss of trust.
In pregnancy cases, mention that gossypiboma can mimic tumors or masses on imaging, complicating diagnosis.
- TOG style flash card for revision on the button below 👇