1. Background & Importance
Sepsis = leading direct cause of maternal death worldwide.
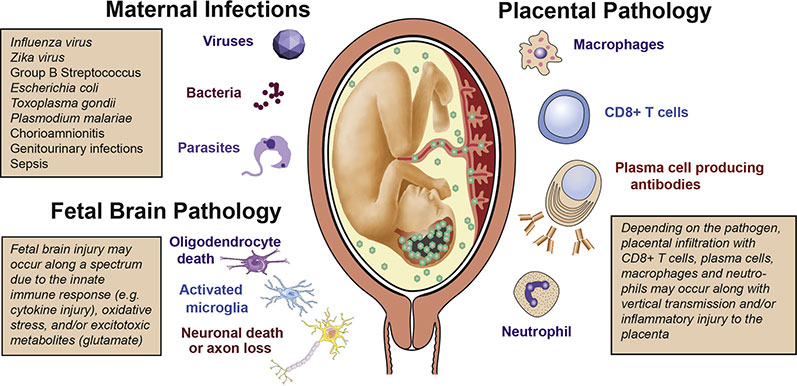
In UK (MBRRACE), Group A Streptococcus (GAS) is the most frequent pathogen in fatal cases.
Other common organisms: E. coli, Klebsiella, anaerobes, MRSA.
Risk factors: obesity, diabetes, immunosuppression, prolonged rupture of membranes, GBS carriage, invasive procedures, retained products.
 2. Definitions
2. Definitions
Sepsis = life-threatening organ dysfunction caused by dysregulated host response to infection.
Septic shock = sepsis + circulatory/metabolic dysfunction requiring vasopressors.
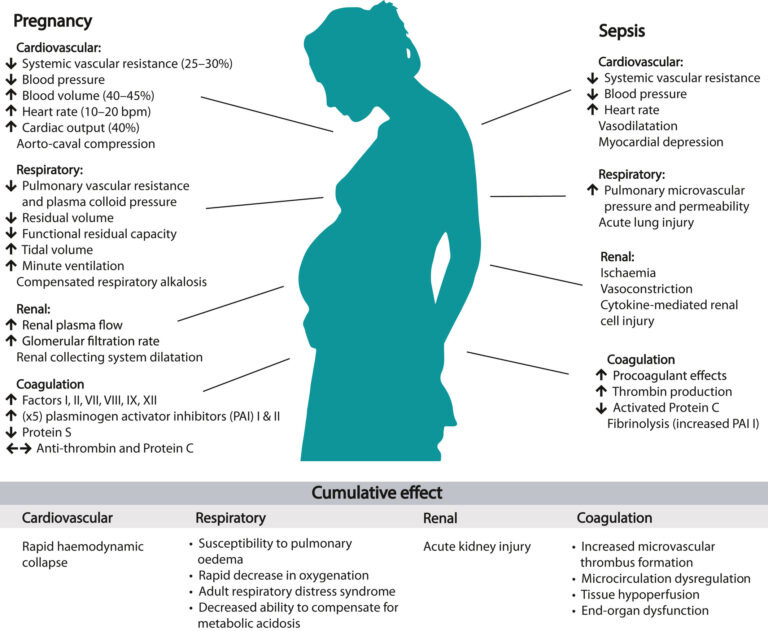
In pregnancy, physiological changes may mask signs (↑ HR, ↓ BP, ↑ WCC).
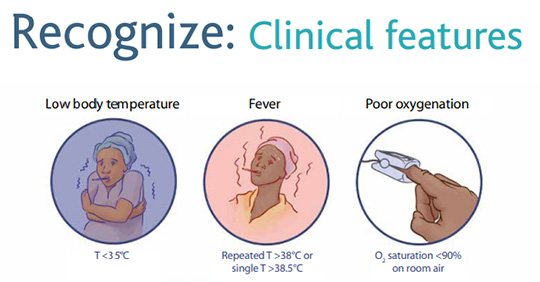
3. Recognition (High-yield)
Clinical features: fever, tachycardia, tachypnoea, hypotension, rigors, altered mental state, oliguria.
Red flags (maternal sepsis six “red” signs):
RR >25/min or SpO₂ <92% on air
SBP <90 mmHg or MAP <60
HR >130/min
New altered mental status
Oliguria (<0.5 mL/kg/h)
Non-blanching rash/lactate >2 mmol/L
 4. Investigations
4. Investigations
Bloods: FBC, CRP, U&E, LFTs, lactate, coagulation.
Cultures: blood cultures before antibiotics, urine, high vaginal/endocervical swabs, wound/pus.
Imaging: CXR/CT/US if source suspected.
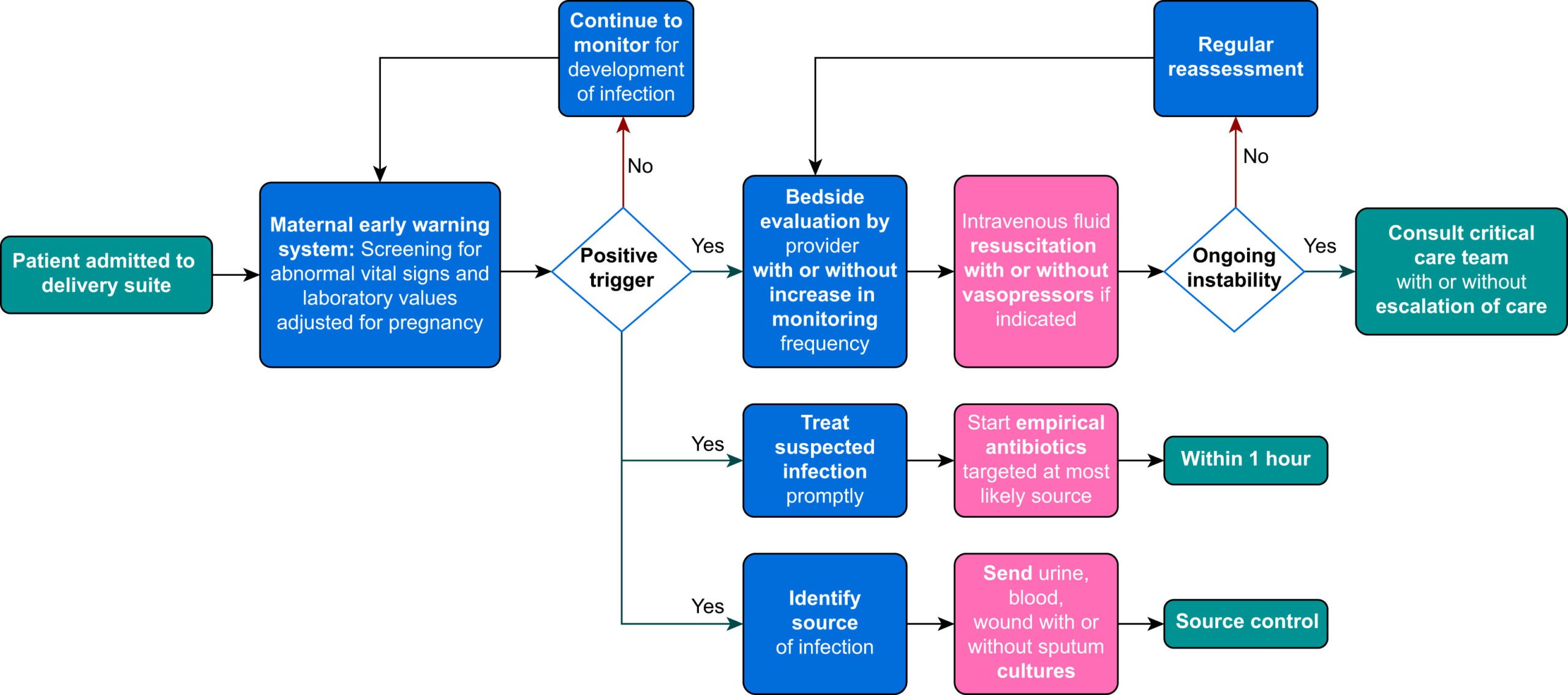
Sepsis screen should be completed within 1 hour of recognition.
5. Immediate Management — “Sepsis 6 in pregnancy”
Within 1 hour:
High-flow O₂.
Take blood cultures.
IV broad-spectrum antibiotics (do not delay).
IV fluids (30 mL/kg crystalloid if hypotensive).
Measure lactate & FBC.
Monitor urine output (catheterise).
Escalate early to senior obstetrician, anaesthetist, microbiology, ITU.
Antibiotics: IV broad spectrum as per local policy (e.g., piperacillin-tazobactam ± clindamycin; consider carbapenem in severe sepsis). Tailor once culture results available.
Surgical source control (evacuation of retained products, drainage of abscess, debridement of wound, removal of line).
6. Obstetric Considerations
Pregnancy: sepsis increases maternal morbidity & mortality; can cause fetal hypoxia, preterm labour, IUFD.
Delivery: urgent if source is intrauterine and woman is unstable; decision multidisciplinary.
Anaesthesia: consider early anaesthetic involvement; avoid neuraxial block if coagulopathy/sepsis.
Antibiotic prophylaxis: given in risk scenarios (PROM, GBS, CS).
 7. Prevention
7. Prevention
Hand hygiene, aseptic technique, timely antibiotics in PROM/chorioamnionitis, minimise vaginal exams.
Immunisation (influenza, pertussis).
Prompt treatment of UTIs.
8. Key Exam Points (MRCOG SAQ/SBA)
Most common cause of maternal death from sepsis in UK: Group A Strep.
First step when suspecting sepsis: Give broad-spectrum IV antibiotics immediately — do not wait for cultures.
Sepsis 6 actions — within 1 hour.
Escalation: involve senior staff, ITU, microbiology early.
Pregnancy physiology may mask sepsis signs → be vigilant.
✅ In summary for exams:
Recognise early — “red flags”.
Treat immediately with Sepsis 6 (antibiotics + fluids = lifesaving).
GAS is the most lethal pathogen.
Escalate, involve multidisciplinary team, and consider urgent delivery if source intrauterine.
For Guideline on Identification and Management of Maternal Sepsis During and Following Pregnancy click below 👇🏼