1. Preconception Care
Offer preconception counselling for women with diabetes.
Target HbA1c < 48 mmol/mol (6.5%) if safe; avoid pregnancy if HbA1c > 86 mmol/mol (10%).
Start folic acid 5 mg daily until 12 weeks.
Stop teratogenic drugs (ACE inhibitors, ARBs, statins).
Screen for retinopathy and nephropathy before pregnancy.
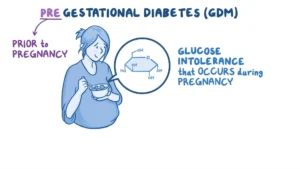
2. Screening for Gestational Diabetes (GDM)
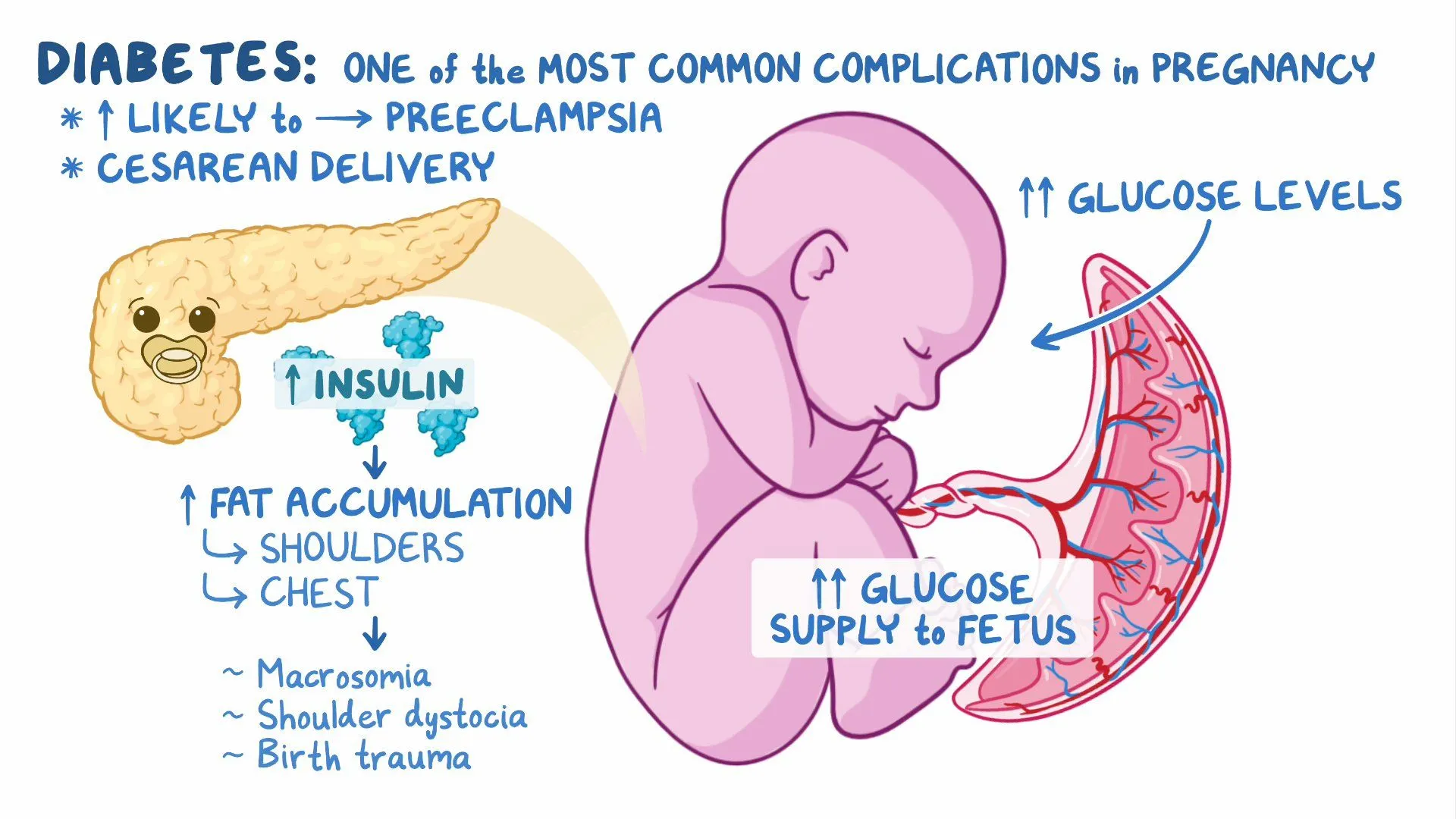
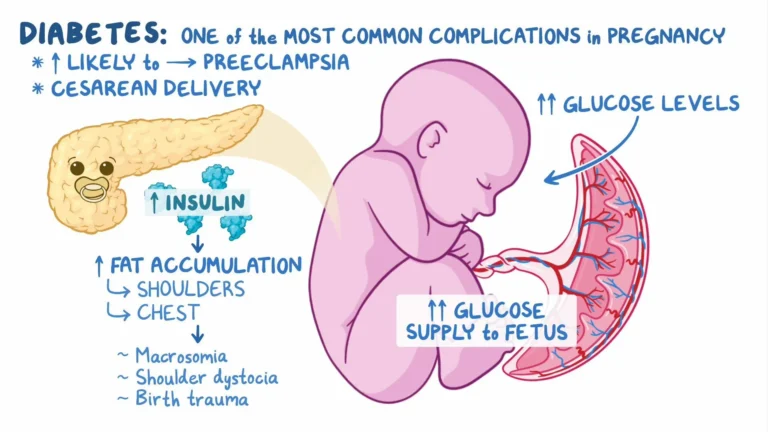
Risk factors: BMI > 30, previous GDM, family history, high-risk ethnicity, previous macrosomia, PCOS.
Offer 75g OGTT at 24–28 weeks for women with risk factors.
Diagnose GDM if:
Fasting ≥ 5.6 mmol/L OR
2-hr ≥ 7.8 mmol/L.
3. Glycaemic Targets in Pregnancy
Fasting < 5.3 mmol/L
1-hour post-meal < 7.8 mmol/L
2-hour post-meal < 6.4 mmol/L
HbA1c every 4–6 weeks for pre-existing diabetes.
Use SMBG (self-monitoring), CGM if indicated.
4. Antenatal Management
Joint care: obstetrician + diabetes team.
Growth scans: 28, 32, 36 weeks.
Retinal checks if pre-existing diabetes.
Treat GDM with:
Diet & exercise →
Metformin (1st line if drug needed) →
Insulin (if inadequate control or contraindications).
5. Intrapartum Care
Maintain maternal glucose 4–7 mmol/L.
Hourly capillary glucose monitoring.
IV insulin-dextrose if required.
Timing of birth:
Type 1 or 2 diabetes: usually by 37–38 weeks.
GDM: usually by 40+6 weeks if no complications not beyond.
6. Postnatal Care
Mother
Stop GDM medications after birth.
Check fasting plasma glucose at 6–13 weeks, then annual HbA1c.
Pre-existing diabetes: reduce insulin after birth, monitor closely.
Contraception & preconception advice for future pregnancies.
Neonate
Feed within 30 minutes of birth, then every 2–3 hrs.
Monitor glucose at 2–4 hrs after birth.
Admit if hypoglycaemia or other complications.
✅ Key Point: Early counselling, tight glucose control, multidisciplinary care, and structured follow-up (for both mother & baby) are central to improving outcomes.
- Click the Below Button to attempt 37 (SBA/EMQs) of above related guideline to prepare for your MRCOG II exam