11. The Investigation and Management of the Small-for-Gestational-Age Fetus and a Growth-Restricted Fetus (RCOG Guideline Summary)
Overview & Scope
Definitions
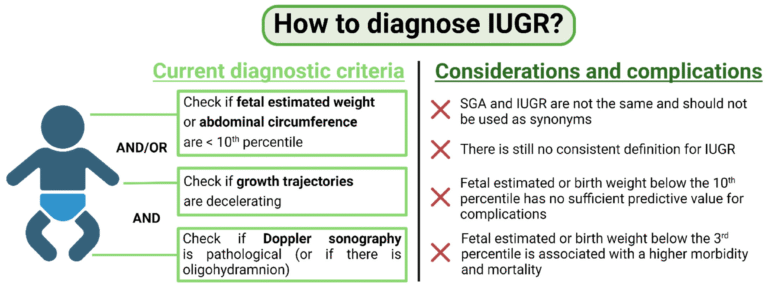
SGA (Small for Gestational Age):
Estimated fetal weight (EFW) or abdominal circumference (AC) <10th centile.Severe SGA: EFW or AC <3rd centile.
Fetal Growth Restriction (FGR): Failure to reach growth potential due to pathology (placental insufficiency, maternal disease, genetic, etc.).
🔹 Risk Factors
Maternal: previous SGA/IUGR, smoking, cocaine, extremes of maternal age, low BMI, chronic disease (hypertension, diabetes, renal, SLE, thrombophilia).
Pregnancy-related: abnormal uterine artery Doppler at 20–24 weeks, PET, APH.
🔹 Screening
Universal fundal height measurement from 24 weeks (plot on customised growth charts).
Serial growth scans for high-risk women (usually 2–4 weekly).
Uterine artery Doppler at 20–24 weeks for women with major risk factors.
Symphysio-fundal height (SFH):
For low-risk pregnancies from 24 weeks.
Plot on customized growth chart.
Ultrasound biometry:
For high-risk women or if SFH < expected.
Use customized growth charts (GROW charts).
Investigations (when SGA or IUGR suspected)
Confirm fetal wellbeing and cause:
Umbilical artery Doppler — most important test.
If abnormal → add middle cerebral artery (MCA) Doppler, uterine artery Doppler, and CPR (cerebroplacental ratio).
Exclude other causes:
Fetal anomaly scan, infection screen (CMV, toxoplasmosis, syphilis if indicated), karyotyping if early or severe.
🔹 Diagnosis (Ultrasound)
Biometry: EFW, AC.
Liquor: oligohydramnios supports diagnosis.
Doppler studies:
Umbilical artery (UA):
Raised PI = placental resistance.
AEDF/REDF = severe placental disease.
Middle cerebral artery (MCA): Brain-sparing if low PI.
Cerebroplacental ratio (CPR): MCA PI / UA PI <1 = high risk.
Ductus venosus (DV): Abnormal if advanced compromise (predicts fetal acidaemia).
Adjunctive Management
Low-dose aspirin (75–150 mg daily) from ≤16 weeks for high-risk women — reduces risk of FGR and pre-eclampsia.
No evidence for bed rest, oxygen therapy, or nutritional supplements.
🔹 Management
Maternal lifestyle: Smoking cessation, control chronic disease, aspirin (for PET prevention if risk factors).
Low-dose aspirin (150 mg daily from 12–36 wks) if risk factors for PET/IUGR.
Do not use: bed rest, oxygen, sildenafil, nutritional supplements (no proven benefit).
Surveillance:
SGA with normal Dopplers → repeat scans 2–3 weekly.
Abnormal Dopplers → increase monitoring (weekly or more).
If UA AEDF/REDF → admit, steroids, daily CTG/Doppler.
Use UA Doppler as primary surveillance tool.
🔹 Timing of Delivery
SGA with normal UA Doppler → deliver at 37 weeks.
SGA with abnormal UA Doppler but present diastolic flow → deliver at 37 weeks.
SGA with absent/reversed end-diastolic flow (AEDF/REDF) →
≥32 weeks → deliver after steroids.
<32 weeks → individualise; continue close monitoring if DV normal, but deliver if DV abnormal/CTG pathological.
Severe SGA (<3rd centile or EFW <500g at viability) → poor prognosis; counsel parents.
🔹 Mode of Delivery
Normal Dopplers → IOL with continuous CTG reasonable.
Abnormal Dopplers (especially AEDF/REDF) → usually caesarean section.
🔹 Key Exam Pearls (MRCOG traps)
Umbilical artery Doppler = best surveillance tool.
MCA and DV are adjuncts, not first-line.
Aspirin is preventive, not curative.
Symphyseal-fundal height (SFH) has poor sensitivity but is used for low-risk women.
Delivery timing is the most tested SBA area: remember 37 weeks for normal UA Doppler SGA, earlier if abnormal.