🚨 Emergency Surgery in O&G — Key Points Guidance
Definition & Scope
Emergency surgery includes unplanned operative interventions in obstetrics/gynaecology (e.g. ruptured ectopic, torsion, ovarian rupture, acute abdomen in pregnancy, postpartum hemorrhage needing laparotomy).
Requires timely decision-making, senior input, multidisciplinary support, and adequate staffing out-of-hours.
System & Organizational Issues (TOG)
Adequate on-call consultant rosters with defined roles (first/second on-call) ensure emergencies are handled promptly.
Units may use regional networks, shared rotas, or consultant “flying squads” for high-risk surgeries.
Quality assurance and audit of emergency surgical outcomes are encouraged.
Focus on communication, transfer protocols, and escalation pathways.
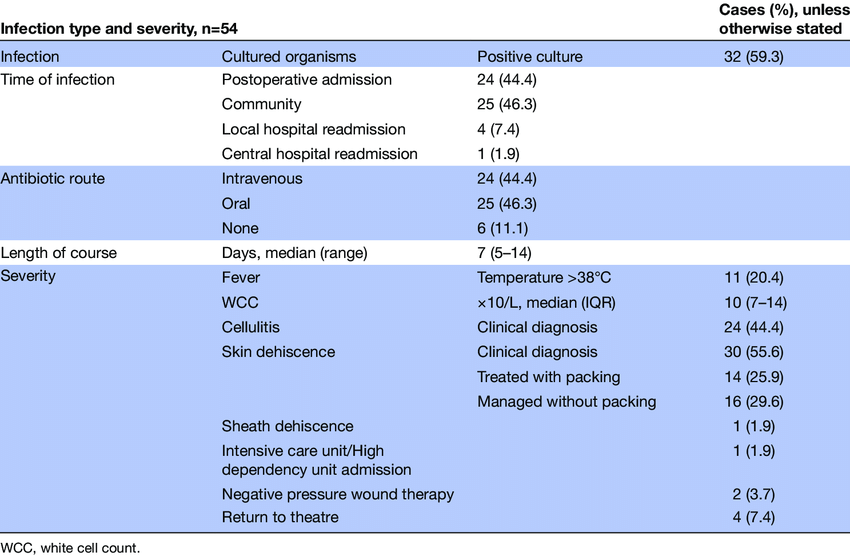
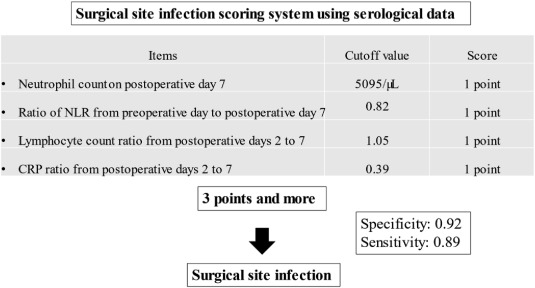
Markers of surgical site infection
Pre-operative Management
IV access × 2 large-bore cannulas
Baseline labs: FBC, U&E, cross-match, coagulation profile.
IV fluids and blood products as indicated.
Antibiotic prophylaxis (broad-spectrum if contamination or ruptured viscus).
Thromboprophylaxis — mechanical if bleeding risk.
Informed consent for possible hysterectomy in obstetric cases.
 Intra-operative Key Points
Intra-operative Key Points
Vertical midline incision preferred in unstable patients.
Assess for concealed bleeding (retroperitoneal, broad ligament).
Minimise delay: rapid suction, pack, identify source, control bleeding.
Blood conservation: cell salvage if available.
Record estimated blood loss.
Clinical Challenges & Risks
High stakes: limited time, unstable patients, less preparation.
Greater risk of complications, bleeding, anesthetic problems, infection.
Surgeons must be prepared for unexpected findings and to convert minimally invasive to open.
Importance of senior involvement in decision-making and operative leadership in emergencies.
MRCOG Exam Tips for Emergency Surgery
In scenarios with unstable patients, illustrate ABCDE, resuscitation, timely decision for surgery, senior involvement.
Mention protocols for safe transfer, surgical safety checklists, pre-op optimization (as far as possible).
For obstetric surgical emergencies, include hemorrhage control measures, damage control surgery, multidisciplinary back-up (e.g. interventional radiology).
Always mention audit, morbidity & mortality review, and learning from complications.
⚠️ Surgical Complications in Gynaecology TOG Highlights
Incidence & Context
Complications in gynaecologic surgery are “considerable,” even in expert hands.
In benign gynaecologic surgery, “major complications” (requiring medical or surgical intervention) may occur in ~ 5 % of cases.
Emergency procedures carry higher odds of complications compared to elective ones.
Types of Surgical Complications
Common categories involve:
| System / Organ | Specific Complication |
|---|---|
| Bowel / GI | Bowel injury, perforation, obstruction, fistula |
| Urinary | Ureteric injury, bladder injury, fistula |
| Vascular / Hemorrhage | Bleeding, hematomas, vascular injury |
| Infection / Sepsis | Wound infection, pelvic abscess, peritonitis |
| Adhesions / Obstruction | Post-op adhesions causing bowel obstruction |
| Anesthetic / Systemic | Thromboembolism, anesthesia complications, DIC |
Example: Laparoscopic entry complications (e.g. bowel, vascular, urologic) are more likely in the phase of blind insertion of trocars.
In RCOG Green-top Guideline No. 49 (on preventing laparoscopic entry-related injuries), serious complications estimated at ~1 per 1,000 procedures; bowel injuries ~0.6/1,000, urological ~0.3/1,000.
Risk Factors for Complications
Emergency surgery
Previous abdominal surgery / adhesions
Obesity / difficult anatomy
Surgeon inexperience / low volume
Complex / advanced disease
Prolonged operative time
Poor preoperative preparation
Recognition & Management Principles
Early recognition is key — unrecognized injuries lead to higher morbidity.
Intraoperative vigilance (inspecting operative field before closure).
Low threshold for intraoperative repair or conversion.
Postoperative monitoring — be alert to signs of leakage, peritonitis, bleeding.
Timely re-operation or intervention if complications suspected.
Multidisciplinary support: urology, general surgery, interventional radiology.
Psychological & Professional Impact
Surgeons often feel distress, guilt, and psychological burden (“second victim”) when complications occur.
Effects include impact on sleep, mental health, relationships.
Younger or less experienced surgeons more likely to suffer greater psychological impact.
Prevention & Risk Mitigation
Good surgical technique, anatomical knowledge, and training.
Use safety checklists, time-outs, and “pause” before critical steps.
Adequate staff, appropriate instruments, and senior supervision.
Preoperative planning: imaging, planning for adhesions or difficult anatomy.
In laparoscopy: adopt entry techniques with lowest risk (optical trocars, open entry where needed).
Audit complications, morbidity & mortality meetings, learning systems.
Exam Tips for Surgical Complication Writing
When asked: list types of complications, risk factors, and how to minimize them.
Use sample vignettes: e.g. post-hysterectomy leaking urine → suspect ureteric injury.
Emphasize prevention, but also early recognition & management.
If asked about surgeon “well-being”, mention psychological distress, support systems, learning from errors.
🧩 Mnemonic — “RAPID” for Emergency Surgery
Resuscitate
Assess (ABCDE)
Prepare for theatre (blood, antibiotics)
Involve senior team
Definitive surgery