Hyponatraemia in Labour – Summary
Definition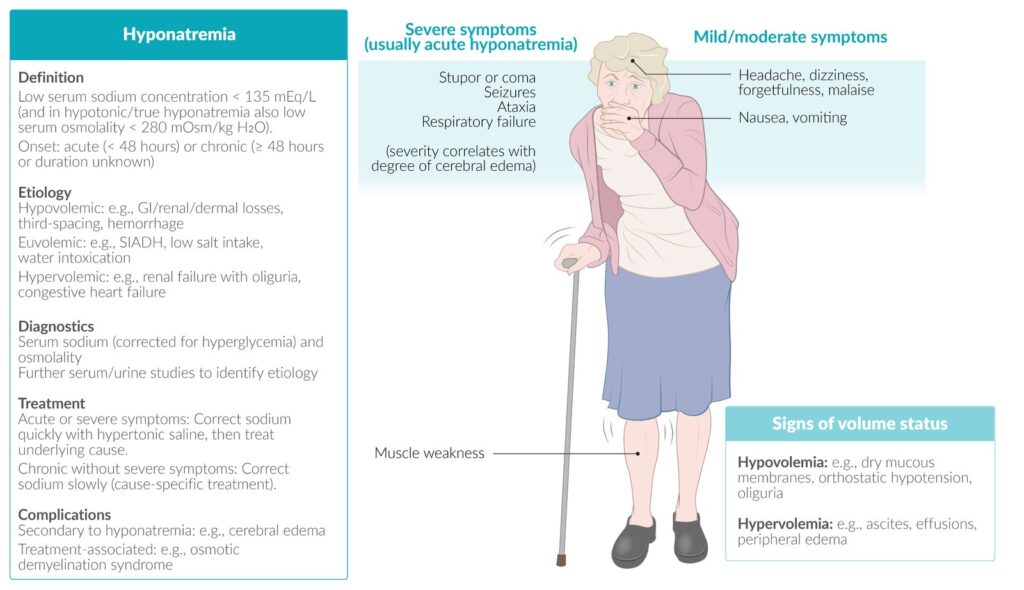
Hyponatraemia during labour is a condition where the plasma sodium concentration falls below the normal range due to water retention, excessive fluid intake, or a combination of both. It can be asymptomatic or life-threatening depending on severity and speed of onset.
Causes
Physiological changes in pregnancy: Lower baseline sodium and plasma osmolality, reduced ability to excrete water.
Oxytocin effect: Endogenous or synthetic oxytocin has an antidiuretic effect (like ADH), promoting water retention.
Excessive fluid intake: Oral or IV hypotonic fluids (e.g., dextrose 5%) can dilute sodium levels.
Prolonged labour: Longer exposure to fluids and oxytocin increases risk.
Risk Factors
Total fluid intake >2.5 L during labour.
Oxytocin infusion for induction or augmentation.
Long or difficult labour.
Impaired ability to excrete free water (pre-existing renal conditions, very young/old maternal age).
Sometimes occurs even in healthy women with high fluid intake.
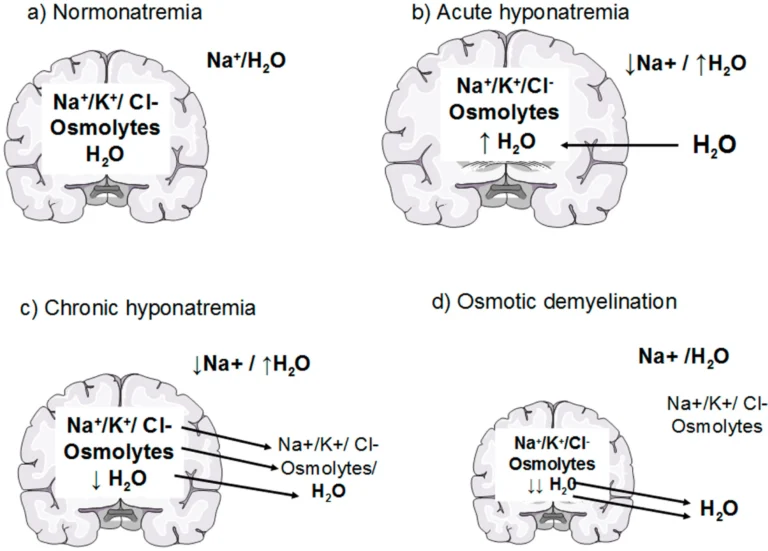
Why it happens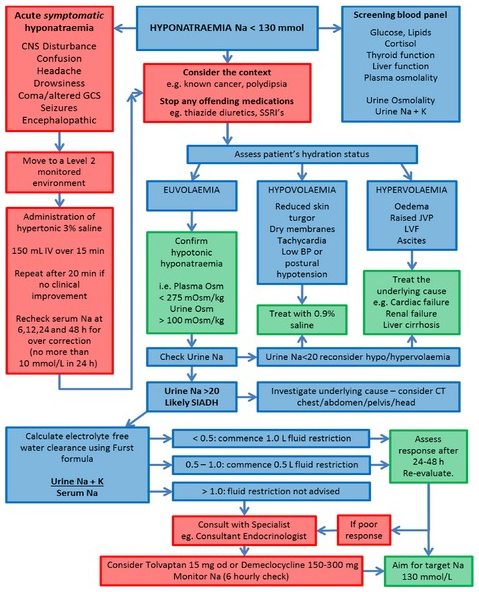
Pregnancy lowers baseline sodium and plasma osmolality, making women more susceptible.
During labour, natural and synthetic oxytocin acts like ADH, causing water retention.
Excessive oral fluids or hypotonic IV fluids (like dextrose solutions) can dilute sodium.
Prolonged labour or large fluid volumes increase risk.
Who is at risk
Women receiving large volumes of IV fluids (>2.5 L) or drinking excessively.
Those on oxytocin infusion for induction or augmentation.
Women with long labours or impaired ability to excrete water.
Sometimes occurs in otherwise healthy women without obvious risk factors.
How it affects mother and baby
Mother: Symptoms range from mild (nausea, headache, lethargy) to severe (confusion, seizures, coma).
Baby: Free water crosses the placenta, so neonatal hyponatraemia can occur, leading to feeding problems, respiratory distress, seizures, or even coma.
Many women are asymptomatic, so risk can be hidden.
Prevention
Monitor total fluid intake and output carefully.
Encourage drinking only to thirst; avoid large amounts of hypotonic fluids.
Prefer sodium-containing IV solutions (e.g., saline, Ringer’s) rather than low-sodium fluids.
Record urine output and check fluid balance regularly.
When to check sodium
If total fluids exceed 2.5 L.
If the woman is on oxytocin infusion.
If clinical symptoms suggest hyponatraemia.
If fluid balance shows significant positive balance.
Management
Mild or asymptomatic cases: Stop excess fluids, restrict water intake, monitor sodium.
Severe symptoms (seizures, coma): Administer hypertonic saline carefully; correct sodium slowly (not more than 12 mmol/L per 24 h).
Neonatal monitoring: Alert neonatal team; observe or test newborn if mother is hyponatraemic.
Avoid rapid correction to prevent complications like osmotic demyelination.
Key points
Even healthy women may develop hyponatraemia if fluid intake is excessive.
Symptom-based detection is unreliable; proactive fluid monitoring is essential.
Prevention is better than treatment: careful fluid management is the most effective strategy.