1. Purpose
To reduce risks and complications associated with laparoscopic entry, especially injuries to bowel and major vessels during blind insertion of needles and trocars.
2. Background & Incidence
~250,000 laparoscopies annually in UK.
Major complication rate: ~1–5 per 1000 procedures.
Most injuries occur during entry before visualization.
Bowel injury: ~1/1000; major vessel injury: ~0.2/1000.
57% of injuries occur during entry.
Higher risk in women with previous laparotomy.
3. Patient Assessment, Counselling, and Consent
Women must be counselled about:
Risks of bowel, urinary tract, and major vessel injury.
Risk of hernia formation at port sites.
Discuss additional risk factors:
Obesity, very low BMI, previous midline laparotomy, peritonitis, IBD.
Must follow RCOG Clinical Governance Advice No. 6 on valid consent.
4. Training
Surgeons must:
Have structured training and supervision.
Be familiar with equipment, instruments, and energy sources.
Work with trained nursing and assisting staff.
RCOG training pathways:
Core Training Portfolio and ATSM in Benign Gynaecological Surgery – Laparoscopy.
5. Entry Techniques Overview
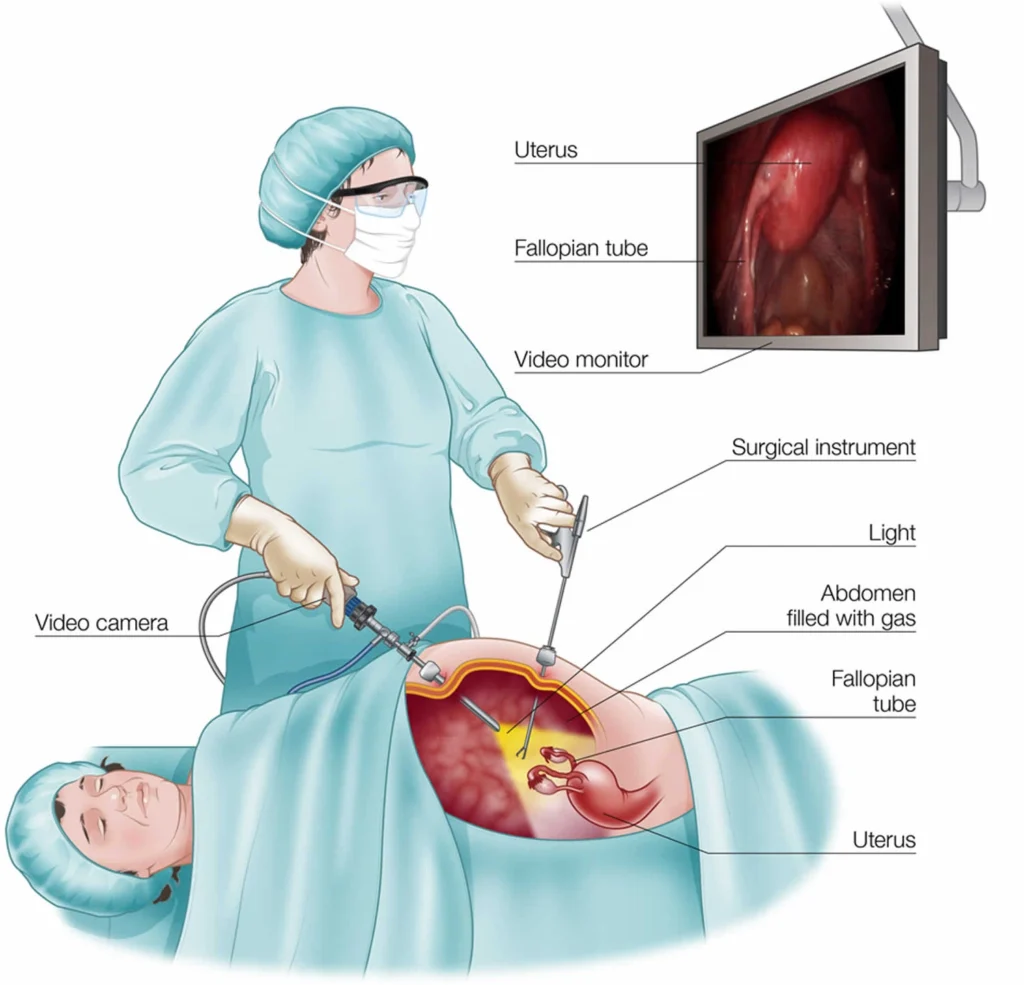
Most complications during laparoscopy occur at the time of primary entry, when access to the peritoneal cavity is first established. There are three main techniques used for this purpose.
The closed (Veress needle) technique is the most commonly employed method, in which a pneumoperitoneum is first created using carbon dioxide insufflation before inserting the primary trocar. While it is widely practiced, this approach carries a risk of blind injury to underlying structures such as the bowel or major vessels.
The open (Hasson) technique involves entering the peritoneal cavity under direct vision through a small incision, allowing the surgeon to visualise the layers being traversed. This method may reduce the risk of major vascular injury but still carries the potential for bowel injury, particularly if adhesions are present.
The direct trocar entry technique avoids prior pneumoperitoneum by inserting the trocar directly into the abdominal cavity. Evidence suggests that it offers comparable safety to the other methods, with no significant difference in major complications demonstrated in randomised trials or meta-analyses. However, some studies indicate that direct entry may be associated with fewer minor complications.
Overall, no single technique has been proven to be significantly safer than the others, and the choice of entry method should depend on the surgeon’s training, experience, and individual patient factors.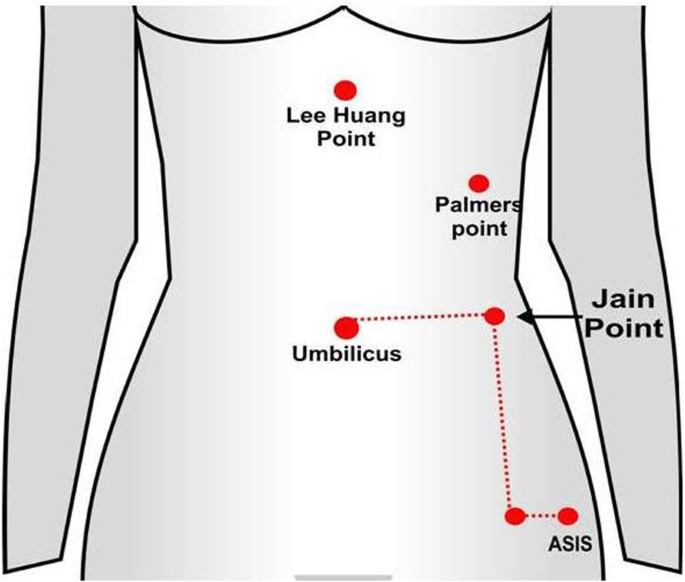
6. Closed (Veress Needle) Technique
Best Practice Steps:
Incision: Vertical at base of umbilicus (not below).
Needle: Sharp, tested spring; ideally disposable.
Patient position: Supine (not Trendelenburg).
Insert needle at right angle to skin; avoid excessive lateral movement.
Confirm peritoneal entry:
Low insufflation pressure (<8 mmHg).
Free gas flow.
Insufflation pressure:
Raise intra-abdominal pressure to 20–25 mmHg before trocar insertion.
Reduces vessel injury by “splinting” effect.
Safe if patient flat; reduce to 12–15 mmHg after trocar placement.
Trocar insertion:
At 90° through base of umbilicus.
Stop immediately upon entry.
Rotate laparoscope 360° to inspect for adherent bowel or haemorrhage.
7. Open (Hasson) Technique
Steps:
Make small incision and enter under direct vision.
Visualise omentum or bowel before inserting blunt trocar.
Anchor fascia with stay sutures; seal with cone.
Insufflate directly through cannula.
Close fascial defect post-procedure to prevent hernia.
Advantage: Avoids blind entry.
Disadvantage: May take longer; risk of gas leak.
 8. Alternative Entry Techniques
8. Alternative Entry Techniques
a) Direct Trocar Insertion
Acceptable alternative; safe in experienced hands.
Meta-analysis: no difference in major complications; may reduce minor ones.
b) Alternative Devices
Visual access trocars and radially expanding trocars may reduce bleeding.
Optical Veress needles: no proven advantage.
c) Alternative Sites
Palmer’s Point (Left upper quadrant):
3 cm below left costal margin, mid-clavicular line.
Use if previous midline surgery or suspected adhesions.
Avoid in splenomegaly or previous LUQ surgery.
Avoid suprapubic, transuterine, or transvaginal entry due to higher risk of injury.
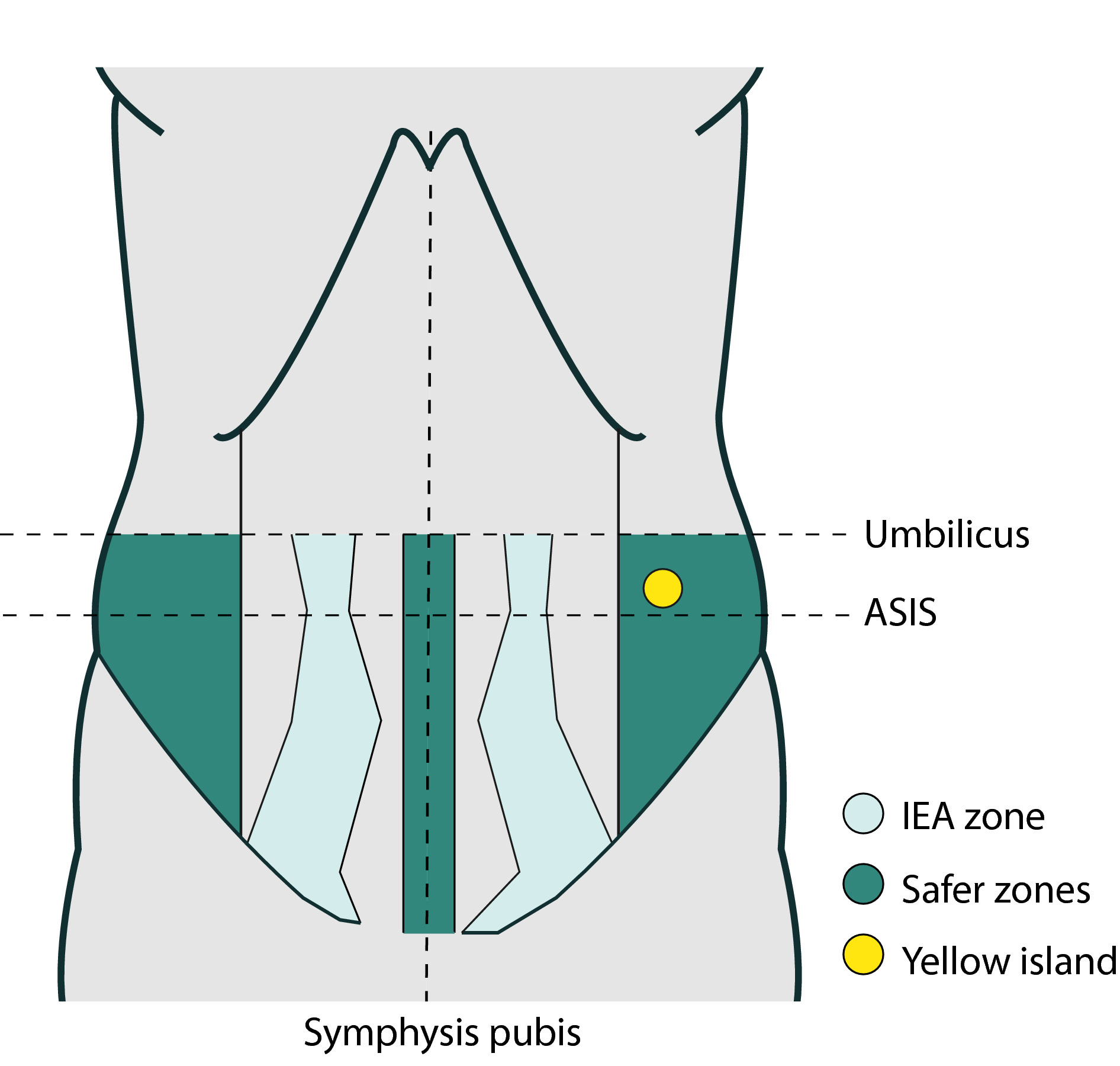
9. Secondary Port Insertion
Always under direct vision.
Maintain pressure at 20–25 mmHg during insertion.
Visualise inferior epigastric vessels to avoid injury.
Remove under direct vision and check for bleeding.
Close fascial defects:
Non-midline ports >7 mm
Midline ports >10 mm → prevent hernia.
10. Special Populations
a) Obese Women
Preferred: Open (Hasson) or Palmer’s point.
If Veress used:
Make incision deep in umbilical base.
Insert needle vertically.
Distance from umbilicus to peritoneum ≈ 6 cm (±3 cm).
b) Very Thin Women
Preferred: Hasson or Palmer’s point.
Aorta may lie <2.5 cm below skin → ↑ vascular injury risk.
11. Documentation and Audit
Auditable Standards:
Documentation of counselling and consent.
Reporting of all adverse incidents and complications.
12. Evidence Levels and Recommendation Grades
A: Meta-analysis or RCT evidence.
B: Controlled but non-randomised studies.
C: Expert opinion or descriptive studies.
Good Practice Points: Based on clinical experience.
Most complications during gynaecological laparoscopy occur at the time of primary entry, which remains the most critical and high-risk phase of the procedure. Entry is required to gain access to the peritoneal cavity for insufflation and introduction of instruments. Various methods are used to minimise the risk of injury, but evidence shows that injuries to bowel, vessels, or other structures most frequently occur before the cavity is visualised. Three main entry techniques are commonly practiced — the closed (Veress needle), the open (Hasson), and the direct trocar entry techniques.
The closed (Veress needle) technique is the traditional and most widely used method. It involves creating a pneumoperitoneum by insufflating carbon dioxide gas into the peritoneal cavity before inserting the primary trocar. The Veress needle is inserted, typically at the base of the umbilicus, until peritoneal entry is achieved, after which gas is insufflated to an intra-abdominal pressure of around 20–25 mmHg to achieve adequate distension. This pressure “splints” the abdominal wall away from the underlying viscera, reducing the risk of vascular injury. The main advantage of this technique is its familiarity and speed, but the major drawback is that the insertion is blind, meaning that the operator cannot see the needle or trocar as it passes through the abdominal wall. As a result, this method carries a higher risk of inadvertent injury to the bowel or major vessels, especially in women with previous surgery, obesity, or intra-abdominal adhesions.
High-Yield Exam Pearls (for MRCOG 2 SBA/EMQs)
| Topic | Key Point |
|---|---|
| Commonest time for injury | During primary entry |
| Safe IAP before trocar insertion | 20–25 mmHg |
| Depth under umbilicus at 10 mmHg vs 25 mmHg | 0.6 cm vs 5.6 cm |
| Preferred entry in obese | Hasson or Palmer’s point |
| Preferred in very thin | Hasson or Palmer’s point |
| Alternative entry site | Palmer’s point (LUQ) |
| Port closure rule | >7 mm lateral, >10 mm midline |
| First sign of vascular injury | Sudden gas flow stop / blood return |
| Commonest organ injured | Small bowel |
Click below for Sba’s on aboce topic exclusively by medisprep 👇🏼