Overview & Scope
Genital herpes in pregnancy is important due to the risk of vertical transmission of HSV to the neonate.
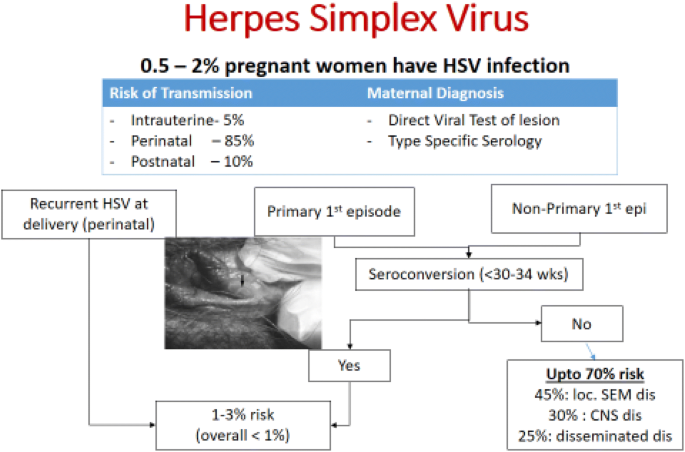
Primary maternal infection (especially in the third trimester) carries the highest risk because maternal antibodies are absent.
Recurrent infection carries a much lower risk since maternal antibodies provide partial neonatal protection.
2. Risks to the Fetus/Neonate
Greatest risk when primary infection occurs in the last 6 weeks of pregnancy (before maternal antibodies develop).
Neonatal HSV can cause:
Skin, eye, mouth lesions
CNS involvement (encephalitis)
Disseminated infection → high mortality
 🔹 3. Antenatal Management
🔹 3. Antenatal Management
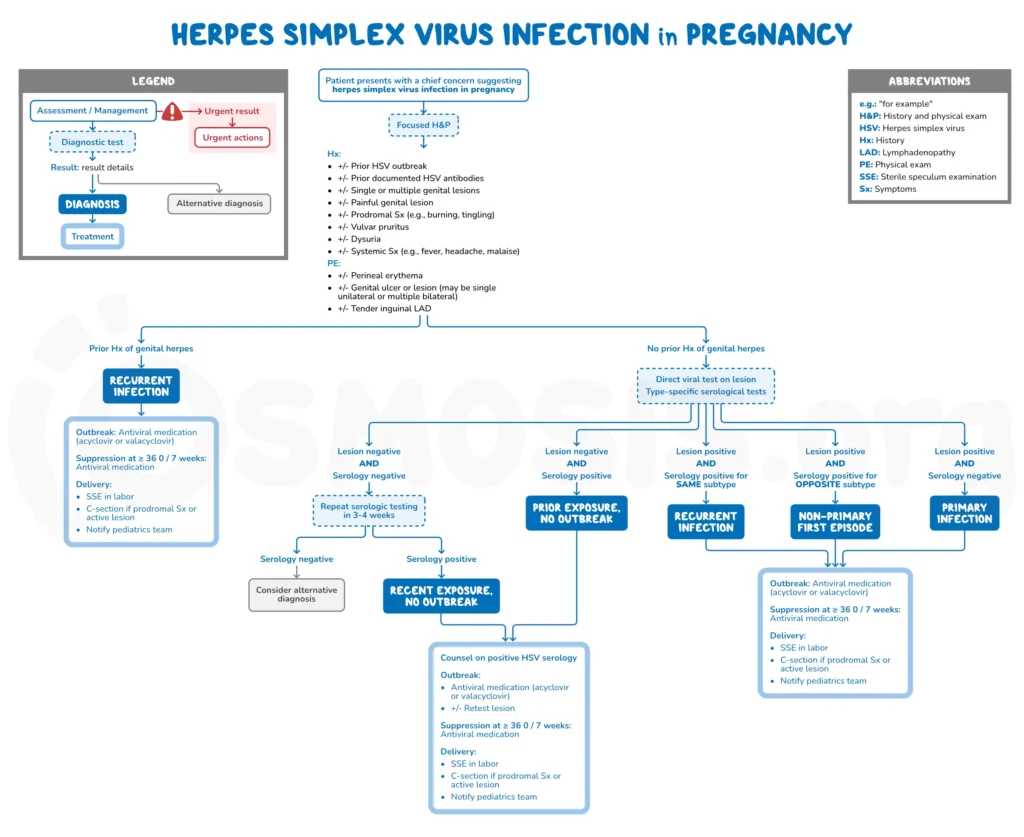
a. Diagnosis
Confirmed by PCR from genital lesions.
HSV-1 or HSV-2 typing is useful for counselling.
Serology may help differentiate primary vs recurrent.
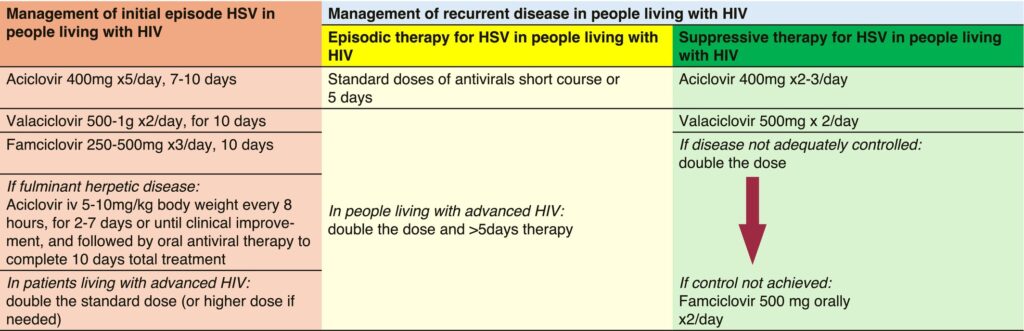
b. Antiviral treatment
Aciclovir is first-line; safe in all trimesters.
Primary infection: aciclovir 400 mg TDS (7–10 days)
Recurrent infection: same dose, shorter course
Valaciclovir may be used (500 mg BD), better compliance.
c. Suppressive therapy
Start at 32 weeks’ gestation (or 22 weeks if high risk / preterm risk).
Aciclovir 400 mg TDS or Valaciclovir 500 mg BD until delivery
➤ Reduces viral shedding and lesion recurrence at term.
Inform neonatal team before delivery.
If primary maternal infection near delivery → neonatal observation & possible aciclovir prophylaxis.
Avoid:
Fetal scalp electrodes
Fetal blood sampling
Instrumental delivery if active lesions
 🔹 5. Postnatal Advice
🔹 5. Postnatal Advice
Transmission risk persists postnatally from direct contact with maternal orolabial/genital lesions.
Advise:
Strict hand hygiene
Avoid kissing baby if orolabial lesions present
Avoid breastfeeding if nipple lesions
🔹 6. Partner Management
Counsel partners; test and treat if symptomatic.
Use condoms and avoid sexual contact during symptomatic episodes.
Updated 2024 guidance (joint RCOG/BASHH) provides changes in diagnosis, suppression timing, management of PPROM, and mode of delivery decisions.
 Exam Tip (MRCOG/FCPS)
Exam Tip (MRCOG/FCPS)
| Topic | Key Point |
|---|---|
| Highest neonatal risk | Primary HSV in last 6 weeks of pregnancy |
| Safe antiviral | Aciclovir (1st choice) |
| Suppression start | Antiviral suppressive therapy to start earlier at 32 weeks of pregnancy for all mothers and pregnant people requiring this, and at 22 weeks if there is a high risk of preterm delivery |
| Delivery if lesions present | C-section |
| Recurrent, no lesions | Vaginal delivery allowed |