Background — Why malposition matters
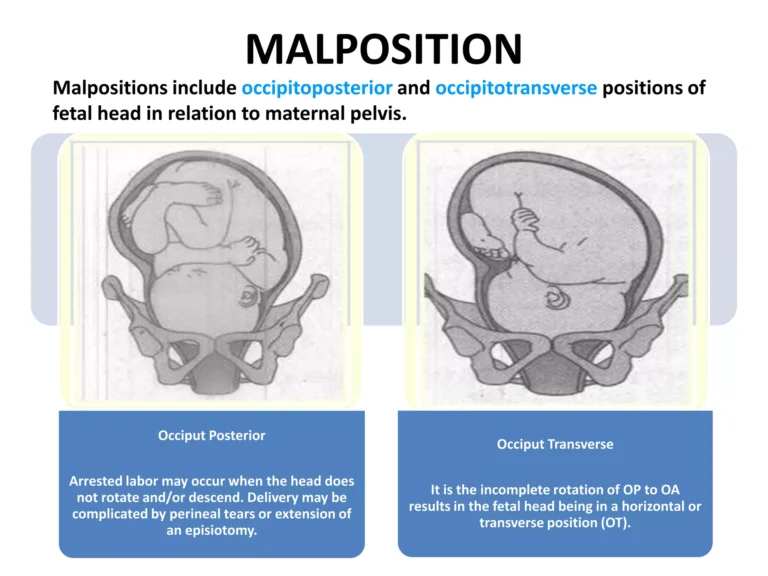
Malposition (e.g. occiput‑posterior (OP) or occiput‑transverse (OT)) means the head is not in the usual occiput‑anterior (OA) orientation; frequently there is associated deflexion of the head or asynclitism. Clinical Gate+2PMC+2
Persistent malposition in the second stage (full dilation) is associated with prolonged labour, increased risk of fetal distress, perineal trauma, higher rates of operative (instrumental or cesarean) delivery. PMC+2pjmhsonline.com+2
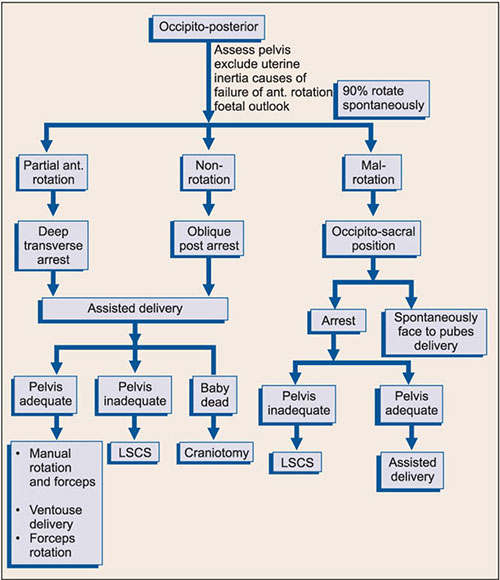
However, many fetuses rotate spontaneously from OP/OT to OA even during second stage. PMC+2ScienceDirect+2
✅ Principles & Initial Approach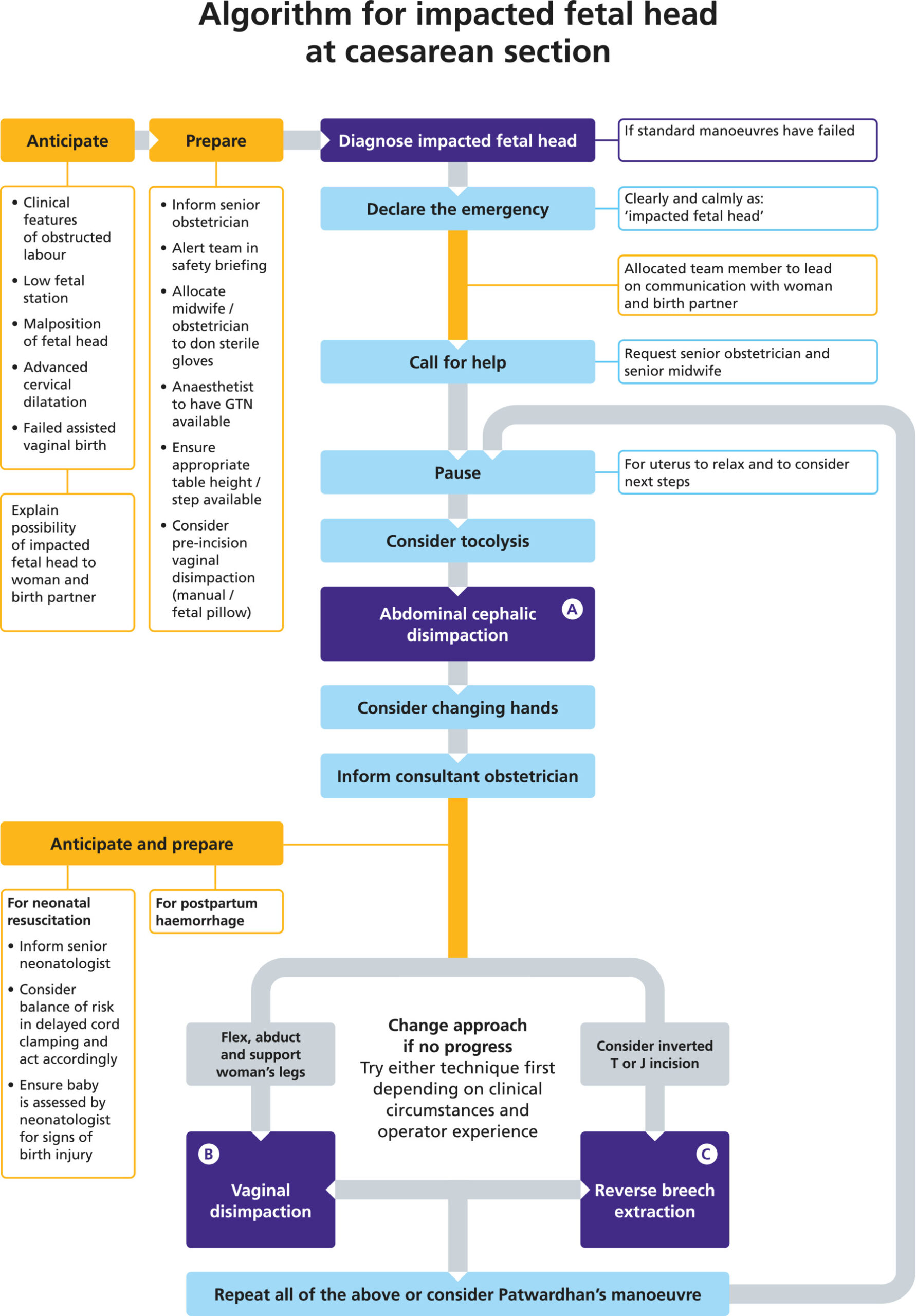
PC: Wiley
Confirm Diagnosis
Clinical vaginal examination remains standard; but due to limitations (e.g. caput, moulding, asynclitism), misdiagnosis is common. blogs.the-hospitalist.org+1
When available, intrapartum ultrasound (abdominal or transperineal) can improve accuracy of fetal head position determination before operative delivery.
Allow time for spontaneous rotation if appropriate
Because many fetuses rotate spontaneously, a period of expectant management (watch & wait) may be reasonable — e.g. 60–90 min in a nulliparous woman, 30–60 min in multiparous — before intervention, provided maternal and fetal condition is reassuring.
During this time, ensure adequate uterine contractions, empty maternal bladder, ensure analgesia/anaesthesia, and monitor progress. ResearchGate+2PMC+2
If malposition persists and delivery is indicated — evaluate options
The main options are:
Manual rotation (to convert OP/OT → OA)
Operative vaginal delivery (rotational forceps or vacuum/ventouse, or direct forceps/vacuum depending on station)
Second‑stage cesarean delivery
The choice depends on: fetal station and engagement, maternal pelvis and soft tissues, fetal size, presence of fetal distress, and experience/skill of the operator.
 🛠️ Management Options
🛠️ Management Options
Manual Rotation
A procedure in which the operator uses hand/fingers to rotate the fetal head from OP/OT to OA. Typically done after full cervical dilatation, with ruptured membranes and empty bladder. PMC+2ResearchGate+2
Techniques vary: either use fingertips on suture lines, or insert whole hand and rotate under parietal bones. PMC+1
If successful, manual rotation may allow spontaneous or assisted vaginal birth, avoiding cesarean or complex instrumental delivery. PMC+2Sieog+2
Evidence: A small RCT (30 women) found no significant difference in operative delivery rate compared to expectant management, and no major adverse events. PubMed+1
A more recent meta‑analysis (2021) reported that manual rotation early in the second stage was associated with a modest (~13 minutes) shorter second stage and no increase in maternal or neonatal morbidity. PubMed+1
Given limited RCT data but favorable observational experience, manual rotation “can be offered” in selected cases of persistent OP/OT.
 Operative Vaginal Delivery (Rotational or Direct Instrumental Delivery)
Operative Vaginal Delivery (Rotational or Direct Instrumental Delivery)
If head is engaged, station acceptable (often at or below ischial spines), and operator is experienced — operative vaginal delivery (OVD) is a well‑established option.
According to a large retrospective cohort (868 women) with persistent malposition: 299 had successful rotational instrumental delivery, while 534 had second‑stage cesarean. PubMed+1
After adjusting for selection bias, neonatal outcomes (e.g. low Apgar, need for resuscitation) were similar between rotational instrument delivery and cesarean; maternal blood loss was lower with instrumental delivery. PubMed+1
Therefore, when performed by skilled operators, rotational or non‑rotational instrumental delivery is a reasonable and often safe alternative to cesarean in second-stage malposition.
However, “heroic” use of force or repeated attempts should be avoided; if progress is not adequate after a few contractions/pulls, conversion to cesarean is advised. Clinical Gate+2pjmhsonline.com+2
Second‑Stage Caesarean Section
Indicated when instrumental delivery is contraindicated / likely to fail — e.g. high station, unengaged head, suspected cephalopelvic disproportion (size mismatch), unfavorable maternal pelvis, macrosomia, fetal distress, or lack of operator skill/experience.
In cases where head deeply engaged and difficult to disimpact (especially at cesarean), techniques such as table positioning (lower table, tilting head-end down), waiting for contraction to cease, attempting to rotate the head to OT and then delivering, or consideration of reverse breech / “pull” method may be used.
Readiness for senior help and possible extension of uterine incision (J or T) should be considered.
📋 Practical “Algorithm” (Simplified)
Confirm full cervical dilatation → second stage. Confirm fetal head position (digital + ultrasound if available).
If OP or OT, and no immediate fetal/maternal compromise → allow reasonable time for spontaneous rotation.
If malposition persists, consider manual rotation (if skilled operator, emptied bladder, adequate anaesthesia). If successful → allow descent and possibly spontaneous or assisted vaginal birth.
If manual rotation not done / fails / not feasible, and head is engaged with acceptable station → operative vaginal delivery (rotational or direct forceps/vacuum) if operator and conditions suitable.
If head is high, unengaged, suspected CPD, macrosomia, unfavorable pelvis, fetal distress, or no provider skilled for OVD → proceed to second-stage cesarean.
During any intervention — ensure maternal bladder empty, good anaesthesia/analgesia, continuous fetal monitoring, maternal monitoring, consent, availability of senior staff, and readiness to convert approaches if progress fails.
⭐ Key Take‑Home Messages
Persistent fetal head malposition in second stage is common and a frequent cause of prolonged labour, operative delivery, and cesarean.
Manual rotation is a simple, low‑risk manoeuvre that can reduce operative delivery rates, though evidence remains limited; it should be considered in appropriate cases.
Operative vaginal delivery, especially by rotational forceps or appropriately applied vacuum/forceps, remains a valid, often underutilized, option when performed by skilled providers — and may reduce maternal morbidity (e.g. blood loss) versus second-stage cesarean. PubMed+2PubMed+2
Cesarean section remains essential when conditions for safe vaginal or operative delivery are not met (e.g. high head station, unengaged head, suspected CPD, fetal distress, macrosomia, pelvic problems).
The decision must be individualized, depending on fetal station/engagement, pelvic anatomy, fetal size, fetal/maternal status, and the expertise of the attending obstetrician.