1) Definitions & classification (high-yield)
Ovarian cyst = any fluid-filled or complex lesion within/on the ovary; can be functional (follicular, corpus luteum), benign neoplastic (serous/mucinous cystadenoma, endometrioma, dermoid), borderline, or malignant. NCBI+1
Adnexal mass includes ovarian and non-ovarian pelvic masses; management depends on age, menopausal status, symptoms, and ultrasound features. ACOG+1
2) Epidemiology & risk
Most ovarian cysts in reproductive-age women are benign and self-resolving; risk of malignancy increases with age (postmenopausal) and certain family histories (BRCA, HNPCC). ACOG+1
3) Important ultrasound features (exam favourite)
Simple unilocular cyst ≤3–5 cm (pre-menopausal) — usually functional; observe.
Complex features that raise concern: solid areas, papillary projections, multilocularity with thick septations, ascites, bilateral solid components, high vascularity on Doppler.
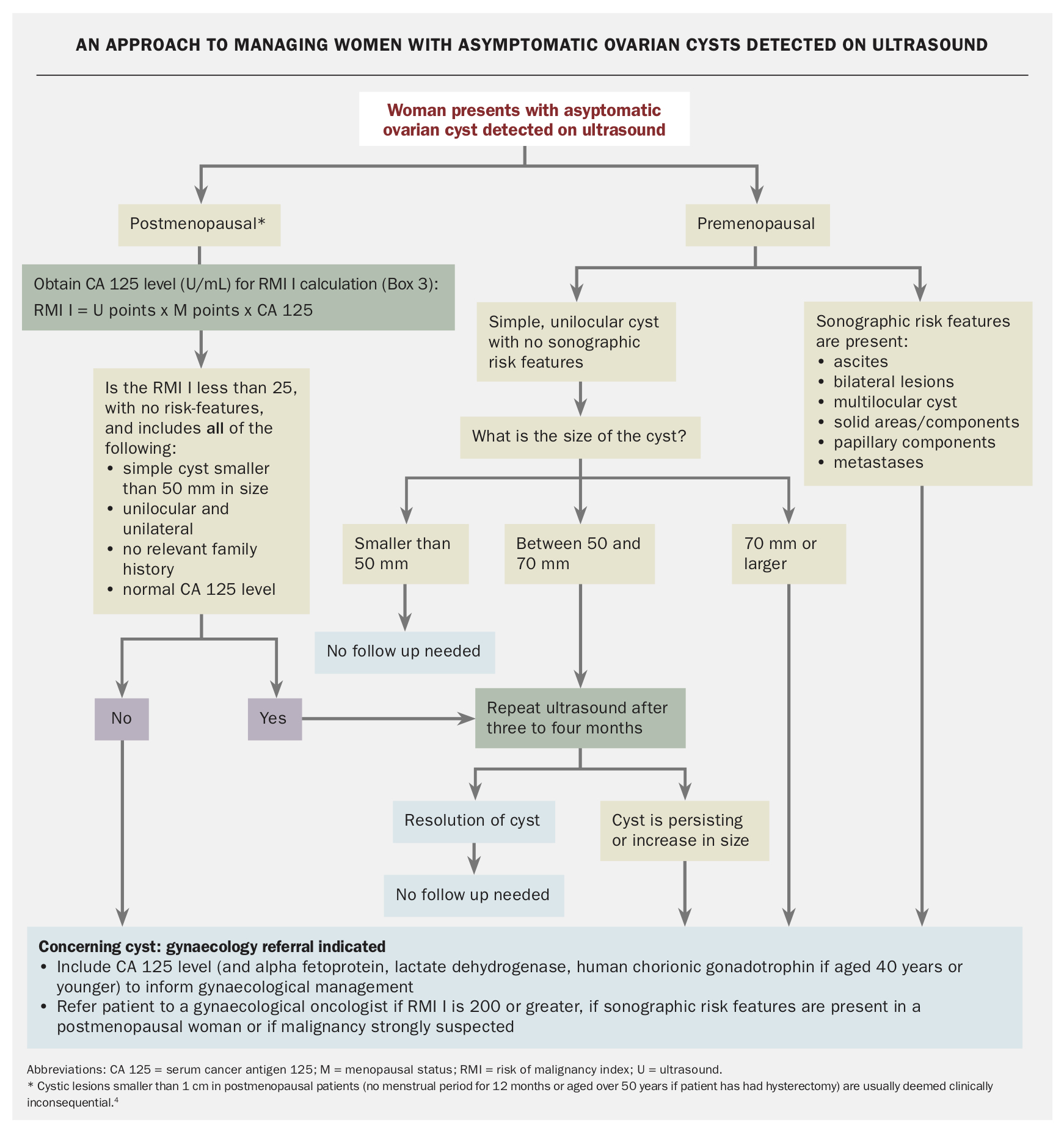
4) Risk stratification tools (memorise)
RMI (Risk of Malignancy Index) = U (ultrasound score) × menopausal status (M) × CA-125. Still widely taught for MRCOG though other models exist.
IOTA ADNEX model and simple rules (IOTA Simple Rules) — higher diagnostic performance; becoming preferred in specialist centers.
5) Tumour markers
CA-125: useful in postmenopausal women and for baseline; nonspecific in premenopausal (endometriosis, fibroids, menstruation raise levels). Use with ultrasound and clinical context.
6) Investigation algorithm (practical MRCOG pathway)
History & exam (age, symptoms, menstrual status, FHx).
Pregnancy test (always in women of reproductive age).
Transvaginal ultrasound (TVS) — first-line imaging for adnexal lesion assessment. If TVS not possible, transabdominal US.
CA-125 in women >40 or if suspicious features; consider other markers for germ cell tumours (AFP, ß-hCG, LDH) in younger women.
Use RMI/IOTA to decide referral to gynecologic oncology vs conservative management.
7) Management — key exam points
Expectant management (serial TVS) for simple, asymptomatic cysts in premenopausal women — many resolve (follow 6–12 weeks to 1 year depending on size/features).
Indications for surgery: suspicious ultrasound features, persistent/enlarging mass, symptomatic (pain, suspected torsion/rupture), postmenopausal complex cysts, very large cysts.
Surgical approach: benign-appearing lesions in reproductive-age women — ovarian-sparing cystectomy if feasible. For suspicious/malignant masses, avoid cyst rupture/spillage, and refer to gynecologic oncology for staging laparotomy or expert laparoscopic oncology where appropriate.
8) Special situations (high yield)
Pregnancy: most adnexal masses are benign and many resolve; surgery reserved for torsion, rupture, or high suspicion of malignancy (laparoscopy usually in second trimester if needed).
Torsion: acute severe unilateral pain; treat as surgical emergency — detorsion and ovarian preservation where possible, even when ovary appears ischaemic. Medscape
Postmenopausal women: lower threshold for referral/surgery; bilateral salpingo-oophorectomy often considered at surgery per guideline recommendations. RCOG+1
9) Ovarian cancer — essentials for MRCOG
Types: epithelial (most common — serous high-grade), germ cell, sex-cord stromal. High-grade serous cancers often arise from the fallopian tube fimbria (important modern concept).
Presentation: vague abdominal symptoms, bloating, early satiety, pelvic pain; red flags = persistent symptoms in women >50 or persistent ascites/weight loss.
Staging: FIGO surgical staging — cytoreductive surgery is key; stage determines prognosis. Adjuvant therapy options include platinum-based chemotherapy, targeted therapy (PARP inhibitors for BRCA/HRD), and maintenance strategies — recent guideline updates cover these systemic options.
10) Exam-style quick revision (flashcards)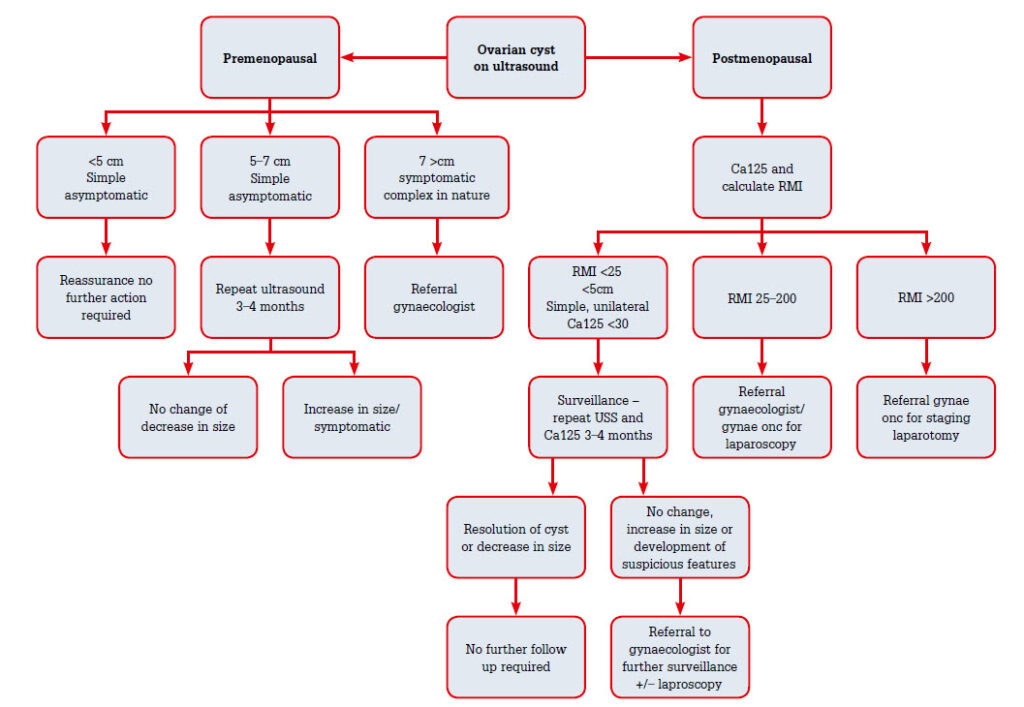
Q: First investigation for adnexal mass?
A: Pregnancy test + transvaginal ultrasound.
Q: Simple ovarian cyst in 28-y F, 3 cm, asymptomatic — management?
A: Expectant management with repeat TVS (likely functional).
Q: Which marker to request for suspected epithelial ovarian cancer?
A: CA-125 (interpreted in context).
Q: Red flag features on ultrasound?
A: Papillary projections, solid areas, septations, ascites.
11) High-yield exam tips (be concise)
Always state age & menopausal status when answering management questions.
Mention pregnancy test for any reproductive-age woman with adnexal mass.
Use ultrasound features + CA-125 + RMI/ADNEX to justify referral/surgery in structured answers
In stable patients with known ovarian cyst and acute pain, urgent pelvic US with Doppler is usually the first step.
If US is inconclusive but torsion still suspected → proceed to laparoscopy.
Management of Suspected Ovarian Masses in Premenopausal Women pdf below