Overview
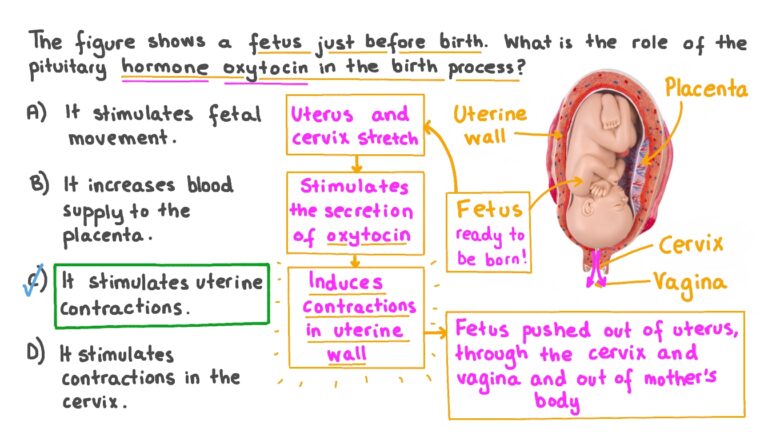
Oxytocin is a naturally occurring hormone used pharmacologically to induce or augment labour by stimulating uterine contractions.
It is a high-risk drug: incorrect use can lead to maternal and fetal complications, including uterine hyperstimulation, fetal hypoxia, and uterine rupture.
2. Indications
Labour induction: for post-dates, pre-labour rupture of membranes, maternal medical indications (e.g., hypertension, diabetes).
Labour augmentation: when labour is slow due to inadequate uterine contractions.
Avoid routine use in normally progressing labour — should not be used simply to accelerate labour or fit schedules.
3. Principles of Safe Use
Start low, go slow: begin with a low-dose infusion; increase gradually.
Target contraction frequency: aim for 3–4 effective contractions per 10 minutes.
Continuous monitoring: maternal vital signs and continuous fetal heart rate monitoring (CTG) are mandatory.
Assess labour progress: vaginal examination every 1–2 hours after starting augmentation.
Stop/reduce infusion if:
Contractions are too frequent (>5–6 per 10 min)
Uterus shows poor relaxation between contractions
Fetal heart rate becomes abnormal
 4. High-Risk Situations
4. High-Risk Situations
Previous cesarean or uterine surgery: increased risk of uterine rupture; use half-dose regimen, with close monitoring.
Multiple pregnancy or malpresentation: caution; oxytocin may worsen complications.
Severe preeclampsia or eclampsia: avoid rapid augmentation due to maternal cardiovascular strain.
5. Potential Complications of Misuse (“Abuse”)
Uterine tachysystole / hyperstimulation → fetal hypoxia, acidosis, neonatal complications.
Uterine rupture, especially in scarred uterus.
Postpartum hemorrhage, due to uterine fatigue or trauma.
Increased instrumental delivery rates.
Fetal distress, low Apgar scores, seizures, perinatal asphyxia.
 6. Monitoring and Safety
6. Monitoring and Safety
Fetal monitoring: continuous CTG throughout oxytocin infusion.
Maternal monitoring: pulse, blood pressure, uterine tone.
Documentation: indication, infusion rate, monitoring, maternal/fetal response, and any dose adjustments.
Escalation: senior review if poor progress, hyperstimulation, or fetal compromise.
7. Key Exam Points
Oxytocin is beneficial when indicated but potentially harmful if used indiscriminately.
Misuse is common in over-medicalized labour or poorly monitored settings.
Correct titration and continuous monitoring reduce risks.
Always assess underlying cause of slow labour before starting oxytocin.
In women with prior cesarean, always use reduced-dose regimen.
Immediate action is required for hyperstimulation: stop infusion, reposition mother, give oxygen, consider tocolysis, senior review.
8. Summary Table: Safe Oxytocin Use
| Aspect | Recommendation |
|---|---|
| Indication | Labour induction or augmentation only |
| Starting dose | Low-dose infusion, gradual titration |
| Target contractions | 3–4 / 10 min |
| Monitoring | Continuous fetal heart rate, maternal vitals |
| High-risk group | Previous CS: half-dose; multiple pregnancy; malpresentation |
| When to stop/reduce | Hyperstimulation, abnormal CTG, poor resting tone |
| Documentation | Indication, dose, response, progress |
The use of intravenous oxytocin for induction and augmentation of uterine activity NHS (UNIVERSITY HOSPITAL WISHAW
WOMEN’S SERVICES DIRECTORATE)