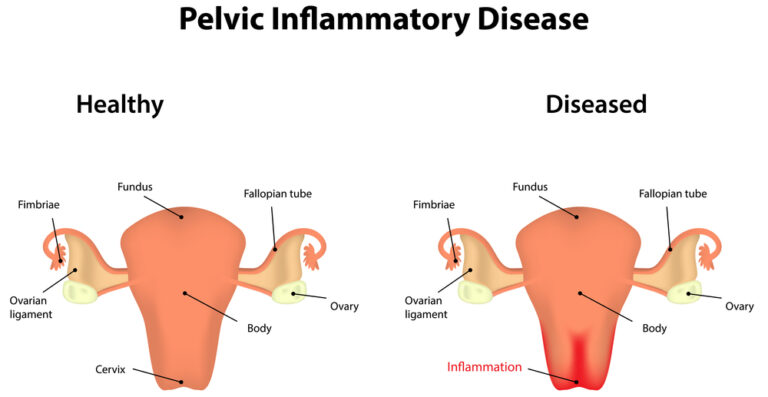
7.1 Microbiological Spectrum and Pathogenesis
Primary Pathogens:
Neisseria gonorrhoeae
Chlamydia trachomatis
Secondary/Co-pathogens:
Anaerobic bacteria (Bacteroides, Prevotella)
Gram-negative rods
Mycoplasma genitalium
Respiratory pathogens (Haemophilus influenzae)
7.2 Diagnostic Criteria Refinement
CDC Minimum Criteria with Modifications
Major Criteria (Must Have Both):
Lower abdominal tenderness
Cervical motion tenderness OR uterine/adnexal tenderness
Supportive Criteria (Increase Specificity):
Oral temperature >38.3°C (101°F)
Abnormal cervical mucopurulent discharge
Presence of WBC on wet prep
Elevated ESR/CRP
Laboratory documentation of cervical infection
Differential Diagnosis Considerations
Ectopic pregnancy
Appendicitis
Ovarian torsion
Hemorrhagic ovarian cyst
Endometriosis
Irritable bowel syndrome
7.3 Treatment Protocols: Detailed Regimens
Inpatient Parenteral Therapy
Regimen A:
Cefotetan 2g IV every 12 hours OR Cefoxitin 2g IV every 6 hours
PLUS Doxycycline 100 mg IV/oral every 12 hours
Transition to Oral: 24 hours after clinical improvement
Regimen B:
Clindamycin 900 mg IV every 8 hours
PLUS Gentamicin loading dose (2 mg/kg), then maintenance (1.5 mg/kg) every 8 hours
Advantage: Better anaerobic coverage for tubo-ovarian abscess
Outpatient Management Criteria
Suitable Candidates:
Mild-moderate clinical severity
Low risk of non-compliance
No nausea/vomiting
Ability to follow up within 48-72 hours
Regimen:
Ceftriaxone 500 mg IM (single dose) – increased dose for gonorrhea resistance concerns
PLUS Doxycycline 100 mg orally twice daily for 14 days
PLUS Metronidazole 500 mg orally twice daily for 14 days
 7.4 Complication Management
7.4 Complication Management
Tubo-Ovarian Abscess (TOA)
Imaging: TVUS for diagnosis, CT/MRI for complex cases
Medical Management: IV antibiotics for 48-72 hours, then oral completion
Intervention Indications:
Rupture (surgical emergency)
Failure to improve after 72 hours of antibiotics
Size >8 cm
Procedures: Image-guided drainage vs. surgical exploration
Fitz-Hugh-Curtis Syndrome
Presentation: Right upper quadrant pain with PID
Pathophysiology: Perihepatitis from ascending infection
Diagnosis: Clinical, confirmed by laparoscopic “violin string” adhesions
Treatment: Extended antibiotic course (14-21 days)
7.5 Follow-Up and Partner Management
Patient Monitoring:
Clinical re-evaluation within 48-72 hours
Test-of-cure for gonorrhea/chlamydia at 3-4 weeks
Screening for reinfection at 3-6 months
Partner Management:
Expedited partner therapy where permitted
Treat all sexual partners within 60 days prior to diagnosis
Abstinence until patient and partners complete treatment
PID – Investigations (Based on RCOG GTG & BASHH 2019)
🧪 1. Diagnosis is primarily clinical
PID is a clinical diagnosis — investigations are supportive.
Do not delay treatment while awaiting test results.
🧬 2. Microbiological investigations
Endocervical and vaginal swabs should be taken before starting antibiotics, if possible:
NAAT (Nucleic Acid Amplification Test) for:
Chlamydia trachomatis
Neisseria gonorrhoeae
Microscopy, culture, and sensitivity for:
Mycoplasma genitalium (if available)
Trichomonas vaginalis (if symptomatic or high-risk)
Bacterial vaginosis and aerobic vaginitis (if discharge present)
Consider urine NAAT if cervical swabs are not feasible.
💉 3. Blood tests
Full Blood Count (FBC) – may show raised WBC.
CRP / ESR – non-specific but raised in moderate–severe infection.
Pregnancy test (β-hCG) – mandatory to exclude ectopic pregnancy.
HIV and syphilis testing – recommended for all women with PID (BASHH).
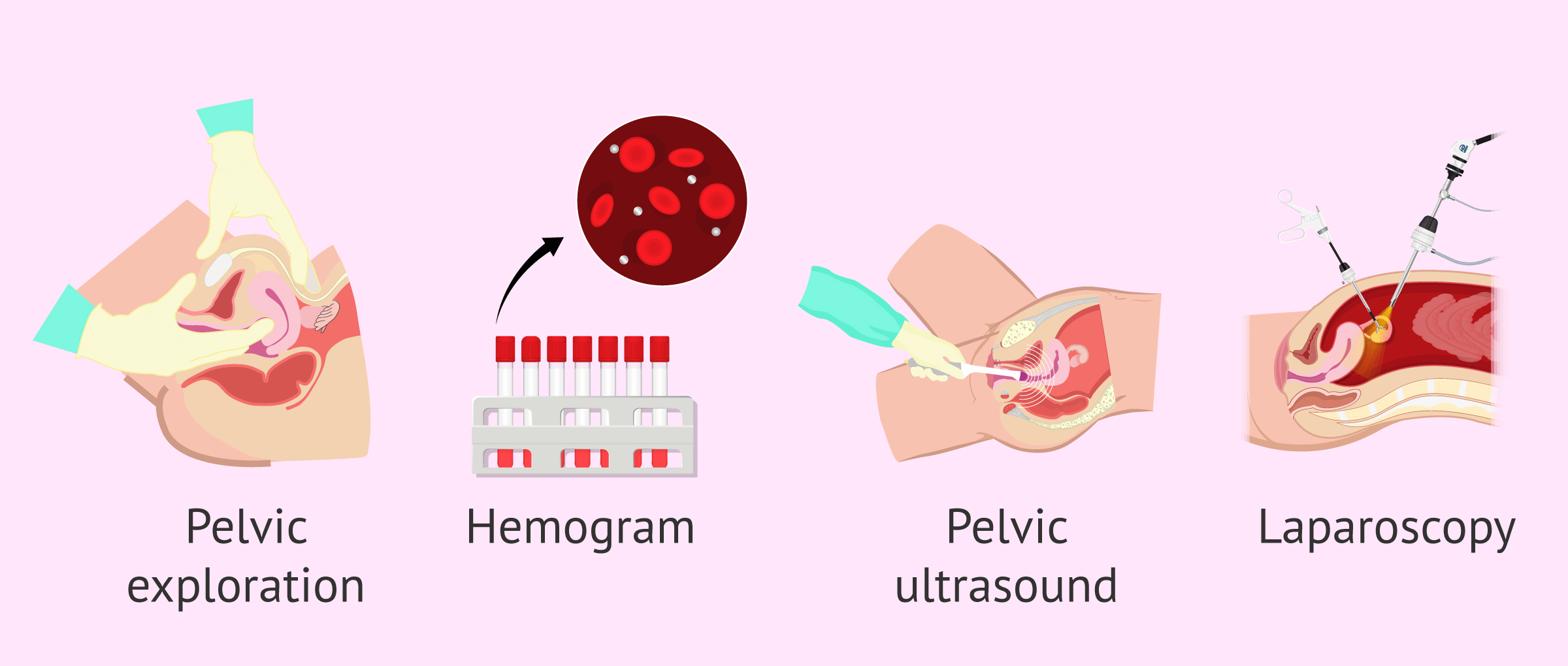
🩻 4. Imaging
Pelvic ultrasound (preferably transvaginal) if:
Diagnosis uncertain,
Adnexal mass or abscess suspected,
No improvement after 48–72 hours of antibiotics.
Look for tubo-ovarian abscess, hydrosalpinx, or free pelvic fluid.
MRI – highly sensitive for complicated PID or diagnostic uncertainty.
CT – if alternative diagnosis (e.g., appendicitis) is suspected.
🔬 5. Laparoscopy
Gold standard for definitive diagnosis, but not first-line/ unless high risk patient.
Indicated when:
Diagnosis is uncertain,
No response to therapy,
Alternative pelvic pathology suspected (e.g., endometriosis, appendicitis).
💊 6. Partner testing and screening
Screen and treat sexual partners for chlamydia and gonorrhoea.
Offer contact tracing and test of cure as per BASHH protocols.
For BASHH guideline on PID click below button