Postmenopausal Bleeding (PMB): Evidence-Based Review
Definition & Importance
PMB: Any uterine bleeding >12 months after menopause.
Incidence: ~10% immediately after menopause.
Endometrial carcinoma risk: 10–15% of women with PMB.
Other causes: Vaginal atrophy, endometrial polyps, fibroids (≈40% of cases).
Cancers to exclude: Endometrial, cervical, vulval.
Key principle:
All women with PMB must be assessed within 2 weeks under the 2-week cancer referral rule.
1. Risk Factors for Endometrial Cancer
Age: <50 yrs (1%), >80 yrs (25%).
Obesity: Risk 18%.
Diabetes: 21%.
Obesity + Diabetes: Up to 29%.
Unopposed oestrogens, PCOS, nulliparity increase risk.
2. First-Line Investigation – Transvaginal Sonography (TVS)
Role: Non-invasive, first-line test to assess endometrial thickness (ET) and morphology.
Cut-off:
≤4 mm: Endometrial cancer unlikely → no biopsy required.
>4 mm: Endometrial sampling required.
Meta-analysis findings:
At 5 mm cut-off, sensitivity 96%, false positive 39%.
Reduces cancer probability from 10% → 1%.
Evidence supports expectant management if ET ≤4 mm and no risk factors.
Follow-up:
If bleeding recurs or image quality poor → proceed to hysteroscopy ± biopsy.
3. Saline Infusion Sonography (SIS)
Enhances detection of intracavitary lesions (e.g. polyps, fibroids).
Accurate but less feasible in postmenopausal women.
Outpatient biopsy or hysteroscopy remain gold standard.
4. Endometrial Sampling
Devices: Pipelle, Vabra.
Accuracy:
Pipelle: 99.6% detection for endometrial carcinoma.
Vabra: 97.1% detection.
Insufficient samples:
If ET >5 mm → reinvestigate (possible missed pathology).
If ET ≤4 mm & hysteroscopy/scan show atrophy → reassure & discharge.
5. Hysteroscopy
Indications:
Inadequate TVS or biopsy.
Persistent bleeding.
Advantages: Direct visualization + targeted biopsy.
Accuracy:
Positive LR: 62.8
Negative LR: 0.15
→ Highly sensitive for endometrial carcinoma.
Outpatient hysteroscopy: Preferred (vaginoscopic approach); inpatient only if difficult or failed.
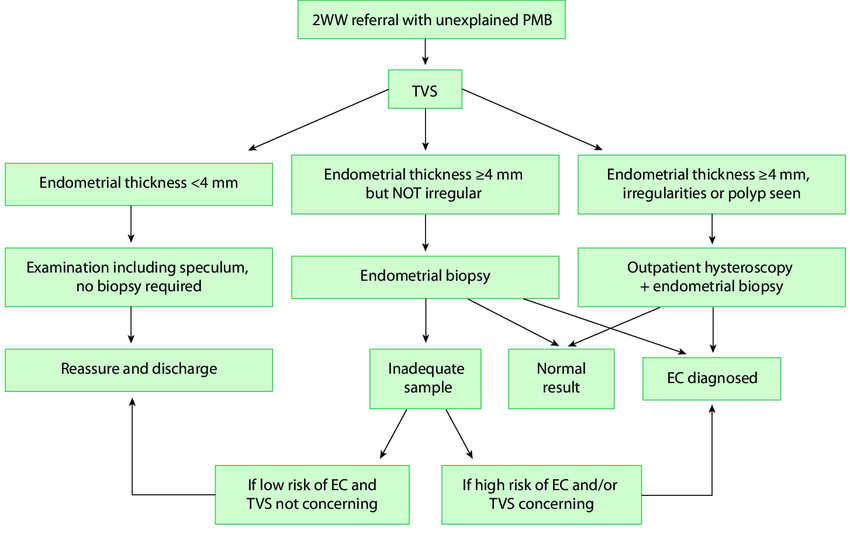
6. Diagnostic Algorithm (Simplified)
Step 1: Exclude non-uterine causes (speculum exam → cervix/vagina).
Step 2: TVS.
ET ≤4 mm: Reassure/discharge (reinvestigate if recurrent).
ET >4 mm: Endometrial sampling ± hysteroscopy.
Step 3:Insufficient sample:
ET ≤4 mm & atrophy → reassure.
ET >4 mm → further investigation.
7. Thickened Endometrium in Asymptomatic Women
Routine screening not justified (low incidence, good prognosis).
From UKCTOCS trial:
Optimum ET cut-off ≈ 5 mm.
Sensitivity 77–80%, specificity 85%.
Endometrial polyps:
Common finding.
Risk of malignancy 0.1% if asymptomatic.
Follow-up only if polyp >18 mm.
8. Endometrial Fluid
If ET >4 mm → may indicate pathology → investigate.
If ET <4 mm → usually benign; no biopsy required.
9. Tamoxifen and PMB
Increases endometrial carcinoma risk 3–6× (up to 4× more with >5 yrs use).
Routine screening not cost-effective.
Investigate only if bleeding develops.
10. Unscheduled Bleeding on HRT
Sequential (cyclical) HRT:
Heavy/prolonged or breakthrough bleeding → investigate.
Continuous combined HRT:
Bleeding after 6 months or after established amenorrhoea → investigate.
Same evaluation pathway as PMB.
11. Endometrial Hyperplasia
Without atypia: LNG-IUS effective & safe alternative to hysterectomy.
With atypia:
14× increased carcinoma risk.
Manage via MDT review; hysterectomy generally advised.
12. Advanced Imaging
3D Ultrasound & Power Doppler:
No superiority over 2D TVS.
Minimal added diagnostic value.
Take-Home Messages
TVS (≤4 mm) reliably excludes malignancy. (may need Endometrial sampling if risk factors)
Endometrial sampling is essential if ET >4 mm or abnormal morphology.
Hysteroscopy allows visual diagnosis and biopsy in one setting.
Asymptomatic thickening rarely needs intervention.
Tamoxifen and HRT users follow same investigation principles if bleeding occurs.
Always reassess for recurrence of bleeding.