Overview & Scope
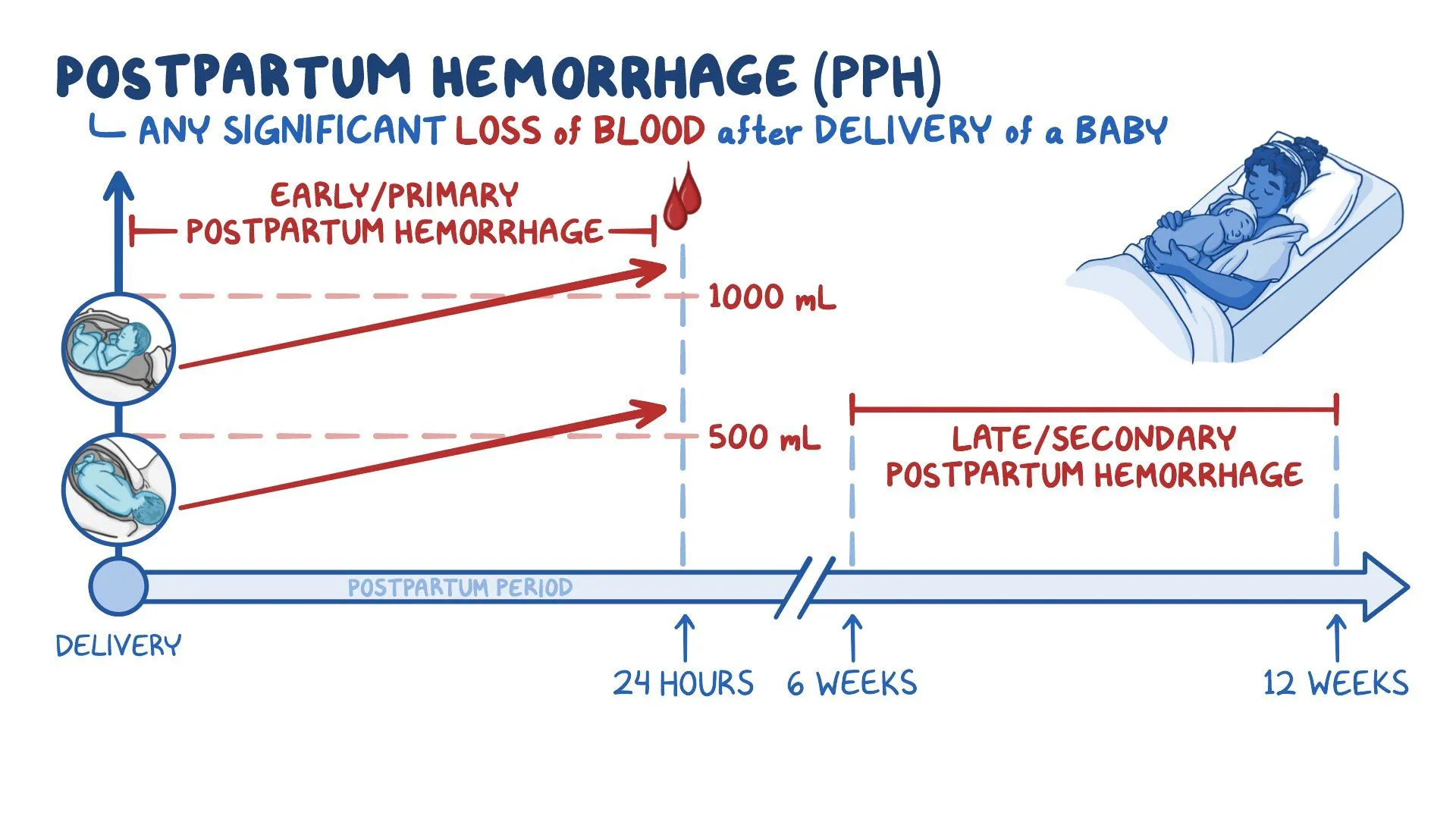
The guideline addresses primary (early) PPH (within 24 hours postpartum) of ≥ 500 mL.
It does not cover antepartum hemorrhage or specialized bleeding disorders in depth. The aim is to provide evidence-based recommendations for prevention, recognition, resuscitation, and escalation of management. RCOG+1
Definitions & Classification
| Term | RCOG Definition | Notes / Comments |
|---|---|---|
| Primary PPH | Blood loss ≥ 500 mL within 24 h of birth | Can be subdivided into minor (500–1000 mL) or major (>1000 mL) |
| Major / Severe PPH | > 1000 mL; sometimes > 2000 mL in clinical usage | Some use >2000 mL to indicate severe / massive hemorrhage |
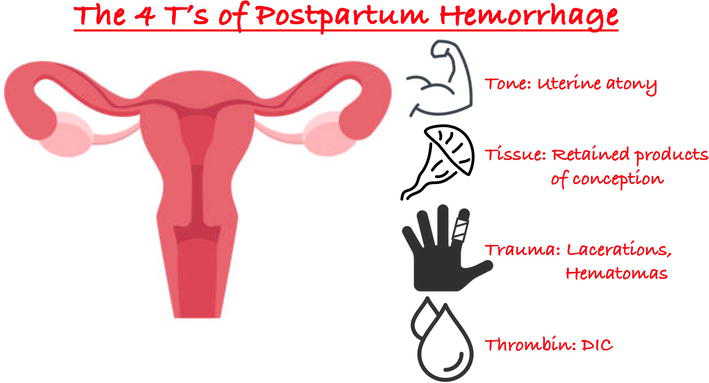
“Four Ts” mnemonic — causes of PPH: Tone, Trauma, Tissue, Thrombin (uterine atony, genital tract injury, retained tissue, coagulopathy)
 Epidemiology & Risk Factors
Epidemiology & Risk Factors
PPH is the most common cause of major obstetric hemorrhage in developed settings.
Many PPH events occur without identifiable risk factors, so universal readiness is essential. RCOG
Risk factors (antenatal, intrapartum, or delivery-related) increase vigilance:
Antenatal / baseline risk factors
Previous PPH
Anemia (e.g. Hb < 9 g/dL)
High BMI / obesity
Multiple pregnancy / polyhydramnios / macrosomia (uterine overdistension)
Hypertensive disease / preeclampsia (coagulation changes)
Placental abnormalities (placenta praevia, accreta spectrum)
Bleeding disorders / anticoagulant therapy
Intrapartum / delivery risk factors
Induction / augmentation of labour
Prolonged labour
Operative delivery (forceps, vacuum)
Caesarean section
Retained placenta / incomplete separation
Genital tract trauma / episiotomy / tears
Chorioamnionitis / intrauterine infection
Use of magnesium sulfate, general anesthesia (uterine relaxation)
Some studies have estimated odds ratios: e.g. placenta previa, abruption, retained placenta carry markedly increased risk.
In exam vignettes, combinations of risk features should ring the alarm for PPH preparedness.
 Prevention & Preparedness
Prevention & Preparedness
Prevention is a central pillar. The RCOG guidelines emphasize Active Management of the Third Stage of Labour (AMTSL) plus system readiness.
Active Management of Third Stage (AMTSL)
Key components:
Routine uterotonic administration immediately after baby born (within ~1 minute)
First choice: Oxytocin 10 IU IM (or slow IV)
If oxytocin unavailable or quality uncertain: alternative agents (e.g. ergometrine, syntometrine, misoprostol, carbetocin) may be used.
Evidence: prophylactic oxytocin reduces risk of PPH by ~60% and need for additional uterotonics by ~50%.
Comparing oxytocin vs syntometrine: efficacy is broadly similar for major PPH prevention, but syntometrine has more side effects (hypertension, nausea).
Controlled umbilical cord traction (CCT) (with counterpressure on uterus) once signs of placental separation are evident. RCOG+1
Early cord clamping (though variable practices)
Uterine massage after delivery of placenta to promote contraction and reduce bleeding.
Evidence supports that AMTSL (vs expectant management) reduces PPH incidence, lowers total blood loss, and reduces need for therapeutic interventions.
Cautions / considerations:
In women at high risk (placenta accreta suspicion, prior PPH, coagulopathy), planning for senior presence, theatre access, blood, etc., is vital—AMTSL alone may not suffice.
Units should maintain PPH kits / hemorrhage carts, protocols, checklists, and conduct simulation drills to ensure rapid, organized response.
Maintain cold chain/storage integrity for oxytocin (degradation at higher temperatures).
Avoid routine episiotomy (unless required), minimize unnecessary trauma.
System Readiness & Risk Stratification
Identify high-risk women antenatally; plan delivery in a facility with adequate resources (blood bank, ICU, theatre) if needed.
Ensure blood group, antibody screen, crossmatch done in advance for high-risk cases.
Maintain equipment readiness: IV fluids, large-bore cannulae, uterotonics, surgical instruments, tamponade devices, sutures, interventional radiology capability (if available).
Conduct regular team training / simulation of PPH emergencies to reduce delays and improve coordination.
Recognition & Early Diagnosis
Early detection of bleeding and physiological compromise is essential because estimates of blood loss are notoriously unreliable.
Monitoring & Indicators
Use cumulative measurement of blood loss, not visual estimation alone.
Frequent vital signs (pulse, BP, respiratory rate, SpO₂), input-output monitoring, assessment of perfusion (e.g. capillary refill, mental status).
Use of Shock Index (SI = HR / Systolic BP): a SI > ~0.9 suggests significant bleeding and correlates better with outcomes than BP or HR alone. (FIGO update)
Early laboratory tests: Hb / Hct, coagulation profile (PT, aPTT), fibrinogen, platelets. Coagulopathy may develop rapidly.
Early Resuscitation Principles
Follow ABCDE principles (Airway, Breathing, Circulation, etc.).
Establish at least two large-bore IV lines, begin crystalloid fluid infusion (e.g. Ringer’s lactate preferred).
Activate massive transfusion / hemorrhage protocols early if indicated (balanced transfusion of RBC, plasma, platelets) to prevent dilutional coagulopathy.
Maintain hemodynamic support (vasopressors if needed) and oxygenation.
Simultaneously investigate and treat the cause (the “T’s”).
Management: Stepwise Escalation Approach
The guideline underscores that interventions often proceed in parallel, not strictly sequentially. The goal is early escalation, rather than waiting for collapse.
Here is a structured therapeutic algorithm:
1. First-line / Medical Therapy
Optimize uterotonics (if not yet given or insufficient):
Oxytocin infusion (e.g. 40 IU in 1 L crystalloid over several hours)
Add second-line uterotonics as needed:
Ergometrine / methylergometrine (contraindicated in hypertension)
Syntometrine (oxytocin + ergometrine)
Prostaglandins: Carboprost (15-methyl PGF₂α) — contraindicated in asthma
Misoprostol (especially useful in low-resource settings)
Tranexamic acid (TXA): administer early (within 3 h of birth) in PPH to reduce bleeding-related death. FIGO supports this strongly.
Uterine massage to encourage contraction and reduce uterine atony.
2. Mechanical / Minimally Invasive Measures
If bleeding persists despite medical therapy:
Uterine balloon tamponade / intrauterine tamponade devices (e.g. Bakri balloon, condom catheter) — a relatively low-risk, effective intervention in many cases.
Uterine compression sutures (e.g. B-Lynch, Hayman, square sutures)
Uterine artery ligation / internal iliac (hypogastric) ligation / uterine devascularization
Uterine artery embolization / radiologic techniques (where available) — can preserve fertility in selected cases
Damage control surgery (packing, staged interventions) may be considered in unstable patients or when definitive surgery cannot be performed immediately. (a concept emphasized in FIGO updates)
3. Emergency Hysterectomy (Definitive)
If bleeding remains uncontrolled after maximal medical and surgical conservative measures, hysterectomy must be done without undue delay. The guideline advises earlier rather than later hysterectomy in life-threatening hemorrhage.
The decision must be balanced with patient’s fertility desires, but in severe hemorrhage, lifesaving is priority.
FIGO / Modern Updates & Bundled Care
Because the RCOG guideline dates from 2016/2017, more recent FIGO recommendations provide enhancements, especially for implementation and resource-stratified settings.
Key FIGO updates:
Bundle approach (“PPH bundles”): standardized packages combining prevention, monitoring, escalation, training, and audits to ensure consistent implementation.
Greater emphasis on Shock Index as a more sensitive early marker of hemorrhagic shock. PMC
Carbetocin: evidence comparing oxytocin vs carbetocin for prophylaxis (especially in cesarean section) is emerging; FIGO includes carbetocin as an alternate uterotonic (100 µg IM/IV) where cost-effective.
TXA: more strongly recommended; FIGO encourages early administration in PPH.
Emphasis on damage control resuscitation principles (combining surgical and resuscitative steps) in extreme PPH.
In low-resource settings, FIGO proposes resource-tailored options (e.g. use of misoprostol, improvised tamponade) where advanced options unavailable.
Pushing for policy, training, implementation, and national adoption of guidelines and protocols.
Key Points & “Must-Know” for Exams
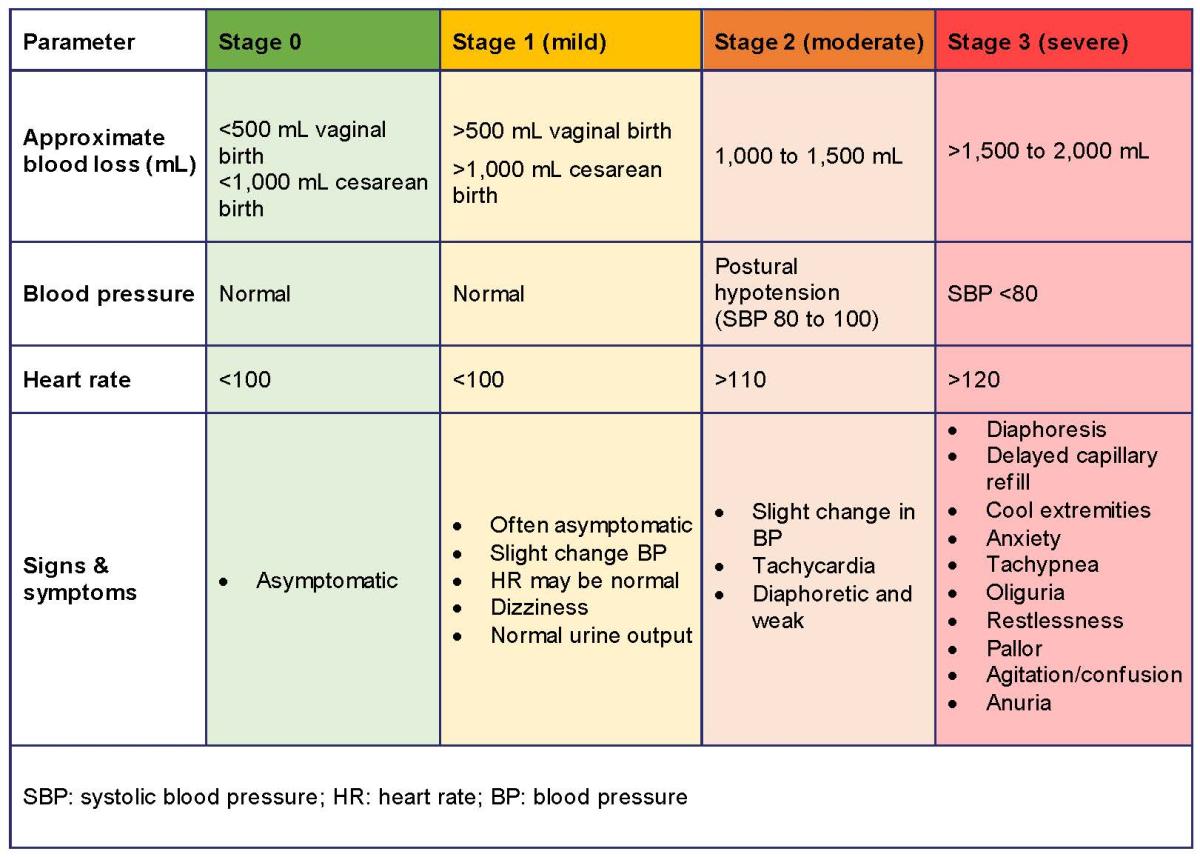
Recognize early signs of PPH; don’t wait for hypotension or collapse to act.
Use Shock Index, trending vital signs, and measured blood loss for early recognition.
Always plan for PPH even in “low-risk” patients because unpredictability is common.
AMTSL is foundational and should be applied to all deliveries unless contraindicated.
Know contraindications for uterotonic agents (e.g. ergometrine in hypertension, carboprost in asthma).
Interventions often overlap in practice — medical + mechanical + surgical concurrently.
Be ready to escalate early; delays cost lives.
In major hemorrhage, maintain resuscitation + hemostasis in parallel — i.e. don’t wait to finish medical therapy before operating.
Hysterectomy is not “last resort after all else fails” — sometimes it must be done sooner in life-threatening situations.
Know the concept of bundle care, simulation drills, system readiness — not just individual procedures.
In low-resource settings, improvised measures (e.g. condom tamponade) may be life-saving — exam vignettes may test knowledge of these adaptations.
When preparing for MRCOG/MCQs, expect clinical vignettes testing: choice & sequence of uterotonics, when to shift to tamponade or suturing, recognizing coagulopathy, contraindications, and timing of hysterectomy.
Prevention and Management of PostpartumHaemorrhageGreen-top Guideline No. 52