Here is a concise but detailed guideline-style summary for retained placenta and the manual removal of placenta (MROP), including definitions, risk factors, indications, preparation, procedure, and after-care. Always conform to your local institutional guidelines and obstetric protocol.
1. Definition & Background
Retained placenta refers to the failure of the placenta to deliver spontaneously or to fully detach within a given time frame after childbirth. PubMed+3PMC+3PMC+3
It is a significant contributor to postpartum haemorrhage (PPH). PMC+1
The third stage of labour (from delivery of baby to delivery of placenta) is prolonged, the risk of haemorrhage increases. PMC+1
Incidence: around 1-3% of vaginal deliveries. PMC+1
2. Risk Factors
Some of the factors associated with retained placenta:
Uterine atony or poor contraction after delivery. PMC+1
Abnormally adherent placenta (eg. placenta accreta spectrum). PMC+1
Preterm delivery, high parity, previous uterine surgery/instrumentation, IVF conception. PMC
Prolonged labour or prolonged third stage. PMC
 3. Prevention / Early Management of Third Stage
3. Prevention / Early Management of Third Stage
Active management of the third stage (uterotonic, controlled cord traction, uterine massage) reduces PPH risk and may reduce retained placenta risk. AAFP+2Tommy’s+2
Monitor the duration of the third stage: delays increase risk. Some data suggest increased risk after ~18 minutes and significantly after ~30 minutes. PMC+1
4. Indications for Manual Removal of Placenta (MROP)
According to guideline sources:
If placenta not expelled and signs of separation not present within 30 minutes (active management) or 60 minutes (physiological management) of delivery. Royal Berkshire NHS Foundation Trust+2Medical Guidelines+2
Immediate indication if there is heavy bleeding/haemorrhage before spontaneous expulsion. Medical Guidelines+1
Suspect retained tissue if placenta appears incomplete or membranes appear missing. library.med.utah.edu+1
 5. Preparation Before MROP
5. Preparation Before MROP
Ensure informed consent and explanation of the procedure, risks and benefits.
Adequate analgesia or anaesthesia (regional or general) given the discomfort and invasiveness of the procedure. PMC+1
Ensure IV access, uterotonic drugs ready, blood products as needed (given risk of haemorrhage)
Monitor maternal vital signs, ensure bladder is emptied (distended bladder may interfere). Tommy’s+1
Prepare for operative theatre if needed (especially if suspicion of abnormal placentation).
Manual Removal of Placenta (MROP) – key points
Indications: placenta undelivered beyond the accepted time, signs of separation but retained, heavy bleeding/haemorrhage in the setting of retained placenta.
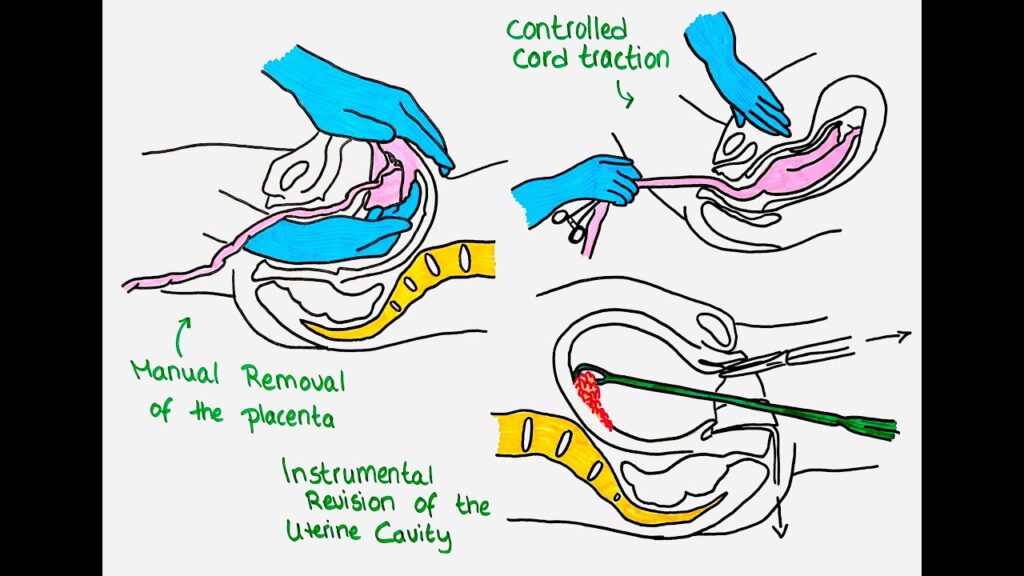
Procedure basics: under adequate anaesthesia/analgesia, one hand on the abdomen stabilising the uterus (fundal support), the other hand (sterile, gloved) inserted into the uterus via the vagina/cervix to gently detach the placenta from the uterine wall, then remove the placenta and membranes, perform uterine exploration for retained clots/fragments, then administer uterotonic agents. Evidence is limited but this is standard practice. PMC+1
RCOG/NICE style recommendations emphasise: “Do not carry out uterine exploration or manual removal of the placenta without an anaesthetic.” NICE
After removal: give uterotonic drugs, ensure the uterus contracts, check for bleeding, inspect placenta and membranes for completeness. Some units recommend prophylactic antibiotics (especially if manual removal done) though practice may vary. Norfolk and Norwich University Hospitals+1
Monitor the woman closely for bleeding, shock, infection.
Summary table of key actionable items
| Action | Details |
|---|---|
| Define time-threshold for retained placenta | 30 min (active) or 60 min (physiological) |
| Ensure third-stage active management | Uterotonic, cord traction (if indicated), uterine massage |
| Assessment when delayed | IV access, check bladder, analgesia, vaginal exam, obstetric review |
| Manual removal indicated when | Undelivered placenta + delay OR separation signs + bleeding OR heavy PPH with retained placenta |
| Manual removal procedure | Under anaesthesia/analgesia, fundal support, intrauterine hand detachment, remove placenta + membranes, give uterotonic, inspect for fragments |
| Aftercare | Monitor bleeding, uterine tone, infection; antibiotics if indicated; document; counsel for future pregnancies |
| Escalation | Suspected placenta accreta → senior obstetric + anaesthetic + theatre involvement |
6. Procedure: Manual Removal of Placenta
Key steps (adapted from MSF / Merck guidelines):
One hand externally cups/supports the uterine fundus through anterior abdominal wall to stabilise uterus. Medical Guidelines+1
Insert the other hand (gloved, sterile) into the vagina, through the cervix, into the uterus. With fingers together, locate an edge of the placenta. Merck Manuals+1
Using the side of your hand/fingers, gently establish a cleavage plane between placenta and uterine wall; detach the placenta by sweeping motion. library.med.utah.edu+1
Once detached, gently remove placenta and membranes via the vagina, taking care to avoid leaving fragments. library.med.utah.edu
After removal, perform uterine exploration—sweep the uterine wall to remove clots, pieces of placenta, membranes. library.med.utah.edu+1
Administer uterotonic drugs (e.g., oxytocin) after removal to encourage uterine contraction. Merck Manuals+1
If cannot easily detach placenta (no cleavage plane) → suspect abnormally adherent placenta (e.g., accreta) → escalate (surgical/hysterectomy) as required. PMC+1
7. After-care and Monitoring
Monitor vital signs, uterine tone, vaginal bleeding frequently (e.g., every 15 min for first 2 h, then every 30 min for next 6 h) as per one guideline. Merck Manuals
Observe for signs of infection (endometritis), retained products of conception (bleeding/discharge), and haemorrhage. PMC+1
Consider prophylactic antibiotics following manual removal (evidence variable). PMC+1
Ensure adequate uterine contraction via massage if needed.
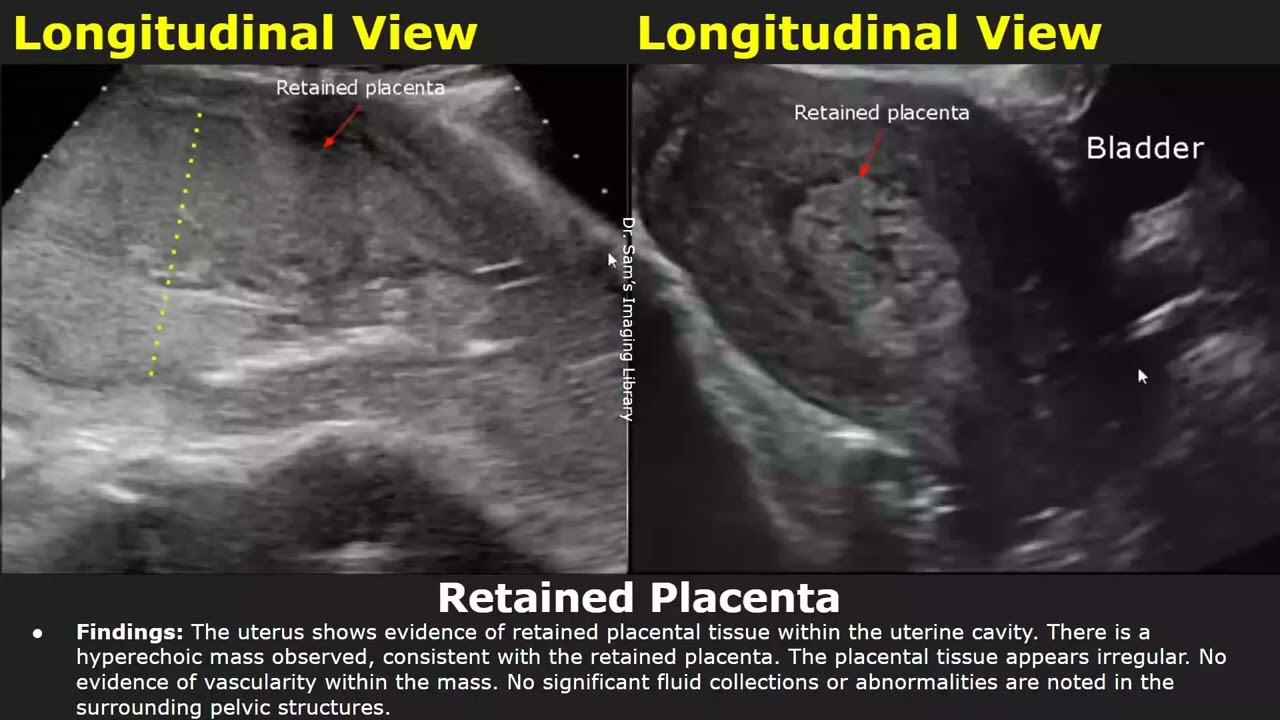
If suspicion of retained fragments, use ultrasound and possible surgical evacuation. PMC
8. Special Considerations
In settings where ultrasound or doppler is available, persistent blood flow between myometrium and placenta may indicate abnormal adherence (placenta accreta) and caution in manual removal. PMC+1
In low‐resource settings, protocolised approach (time limits + early intervention) may reduce morbidity. PMC
9. Summary Flowchart (Simplified)
Treatment of retained placenta*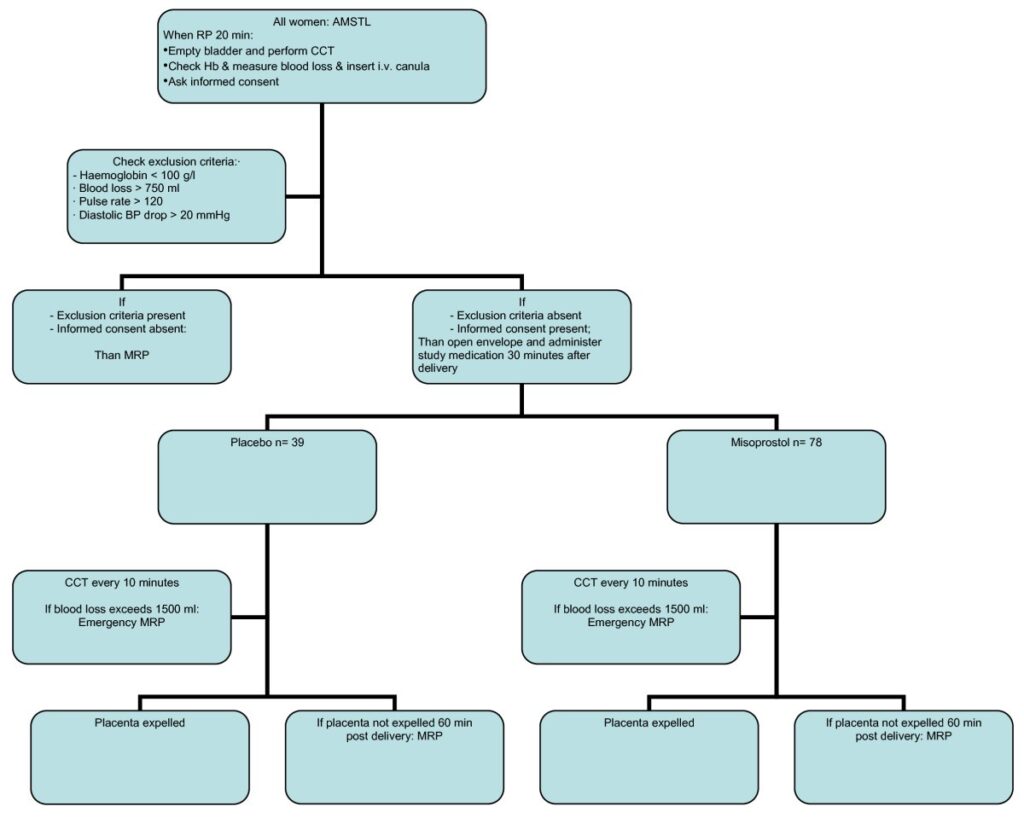
After baby born → apply active management of third stage → monitor for placenta separation.
If no separation or placenta not delivered by ~30 minutes (active) or ~60 minutes (physiological) or there is significant bleeding → prepare for manual removal.
Conduct MROP under anaesthesia → uterine support + manual detachment + removal → uterotonic.
Monitor postpartum closely, intervene further if bleeding persists or retained tissue suspected.
10. Local Implementation Tips
Establish unit‐specific protocol: define time thresholds (30 minutes vs 60 minutes) and trigger for escalating to MROP.
Ready surgical/anaesthetic team if suspicion of adherent placenta.
Ensure uterotonics, blood products, resuscitation equipment are available.
Keep detailed documentation (time placenta expected, actions taken).
Post‐procedure debrief: how time intervals, uterine tone, bleeding behaved; plan for follow‐up.
Placenta Praevia and Placenta Accreta: Diagnosis and Management (Green-top Guideline No. 27a)
Surgical Management of Miscarriage and Removal of Persistent Placental or Fetal Remains Consent Advice No. 10 (Joint with AEPU)